Download to read offline
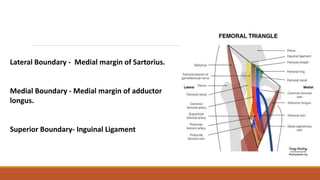
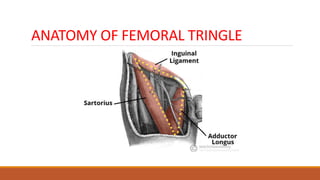

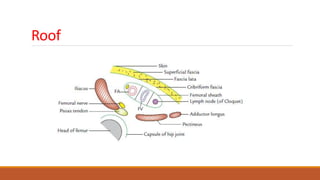

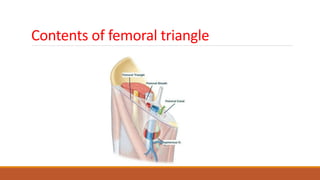
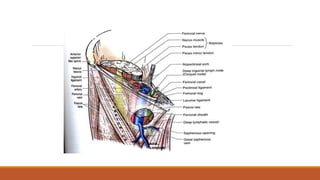
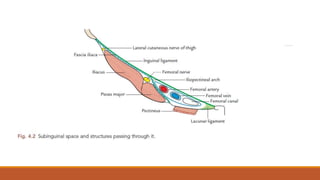
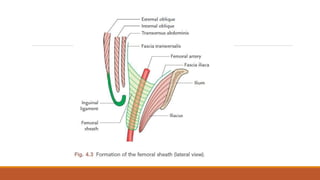
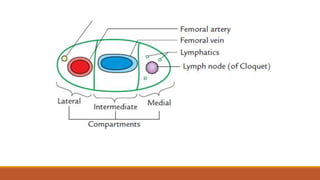
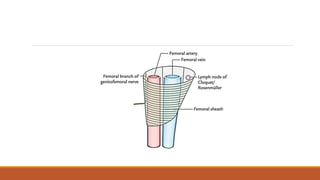

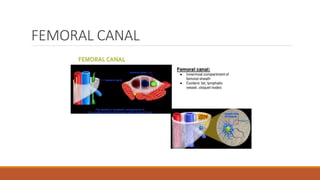
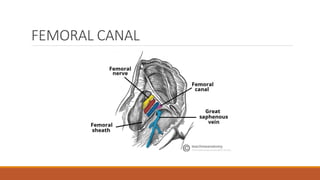

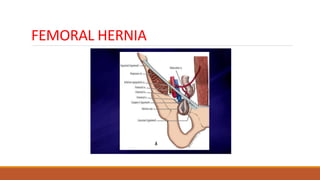
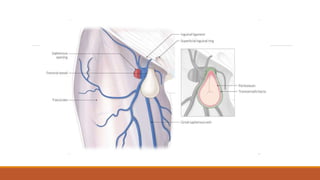
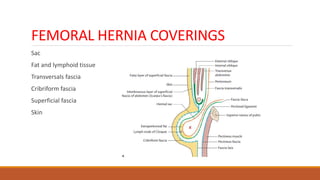
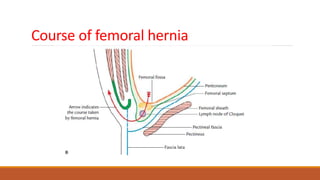
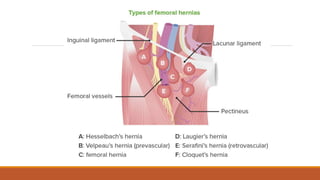
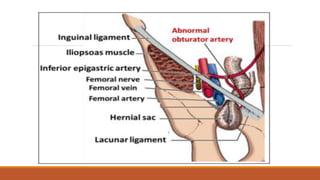
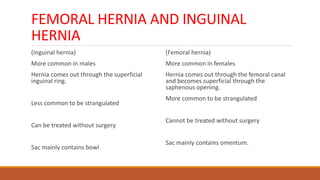
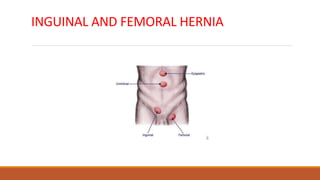
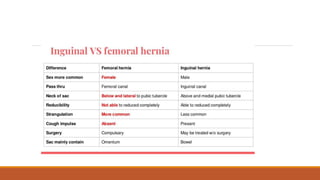
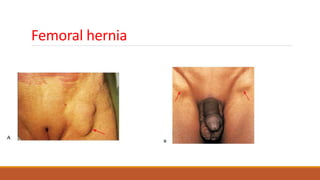





The document discusses the anatomy of the femoral triangle, including its boundaries, contents such as the femoral sheath and canal, and the characteristics of femoral hernias. It explains that femoral hernias, more common in women, involve protrusion through the femoral canal and outlines types and management options for such hernias. Additionally, it includes clinical vignettes and multiple-choice questions to assess understanding of femoral hernias and their differential diagnosis.