Download to read offline














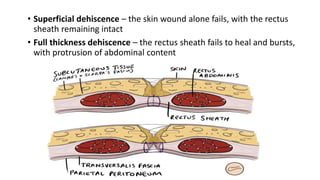


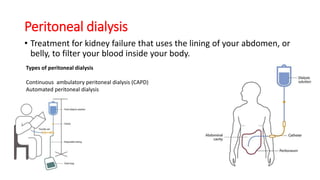
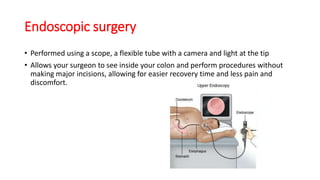


The document outlines objectives and principles for abdominal wall and incision techniques, including various types of incisions used for specific surgeries. It highlights complications associated with these incisions, such as nerve injury and wound dehiscence, and describes procedures like laparoscopic surgery, suprapubic catheterization, and peritoneal dialysis. Additionally, it provides insights into incision techniques like the Kocher, Pfannenstiel, and others, emphasizing muscle-splitting approaches and the importance of maintaining blood supply.























































































