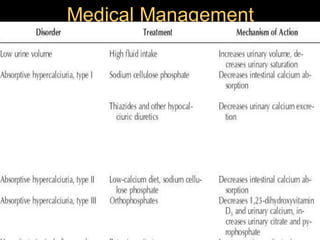
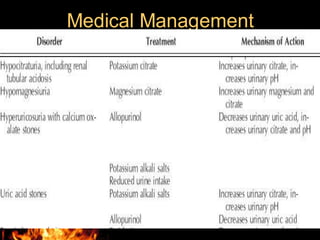
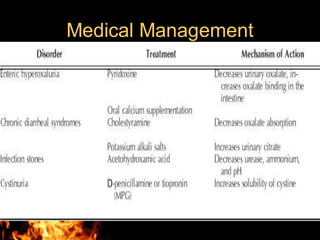
This document outlines the evaluation and management of urolithiasis by the Department of Urology at Govt Royapettah Hospital and Kilpauk Medical College in Chennai. It discusses the moderators, evaluation including history, examinations, imaging and laboratory tests. Management is covered including general measures, medical management, extracorporeal shock wave lithotripsy, endoscopic procedures like ureteroscopy and percutaneous nephrolithotomy, and open surgeries. Indications and complications of the different treatment methods are also provided.













































![Urolithiasis presented by Dr Muhammad nouman([Autosaved]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/urolithiasisautosaved-1-250603143258-c924c676-thumbnail.jpg?width=640&height=640&fit=bounds)














































