Downloaded 15 times





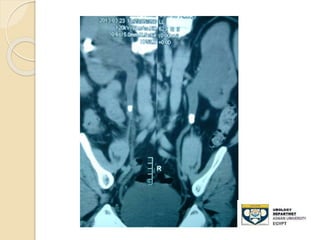






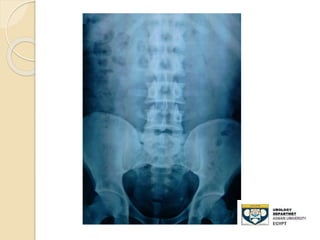






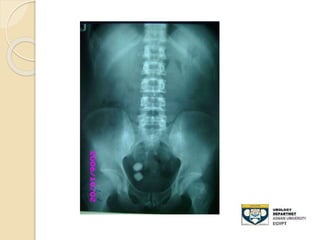


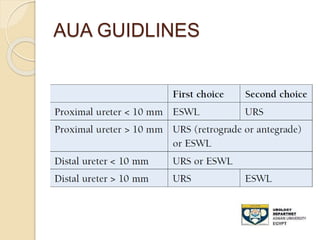


This document provides an overview of the evaluation and management of ureteric stones. It discusses the typical signs and symptoms of ureteric stones including flank pain radiating to the groin. Imaging options like ultrasound, KUB, CT are outlined. Treatment depends on factors like stone size and location, and may include pain control, conservative management, medical expulsive therapy, or active stone removal procedures like ESWL, URS, or PCNL. Prevention emphasizes adequate hydration and dietary modifications.























































































