Download to read offline


















The document provides an overview of urinalysis, including definitions, indications for testing, and methods for collecting urine samples. It covers macroscopic, chemical, and microscopic examinations, detailing the significance of various findings such as color, odor, and specific gravity. The importance of urine analysis in diagnosing kidney diseases, monitoring diabetes, and screening for other health issues is emphasized.
Introduction to urinalysis and overview of topics including urine definition and examination methods.
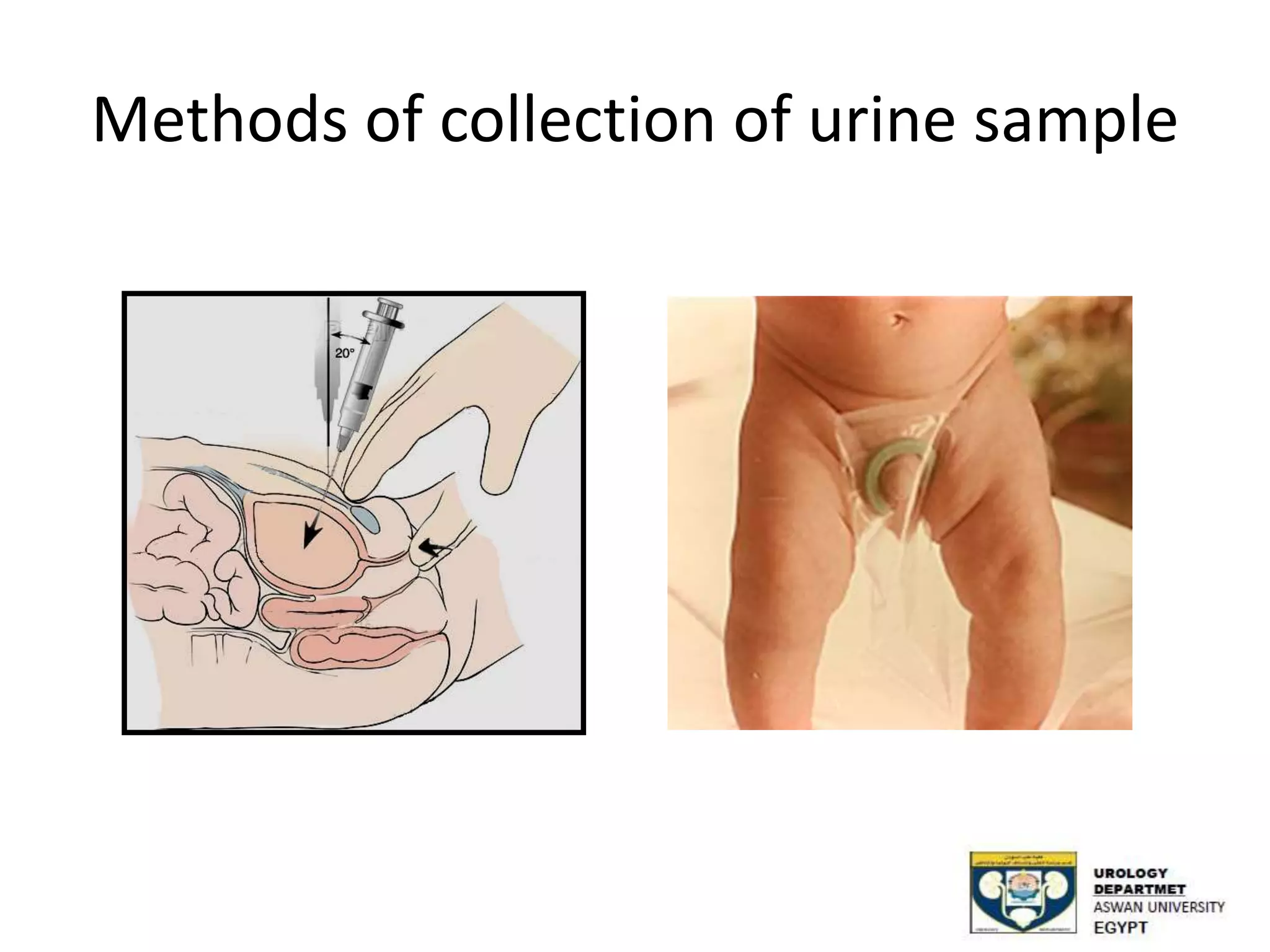
Urine as a product of plasma filtration, its composition, indications for urinalysis, and sample collection methods.
Different examination methods including macroscopic assessment focusing on odor, color, and appearance of urine.
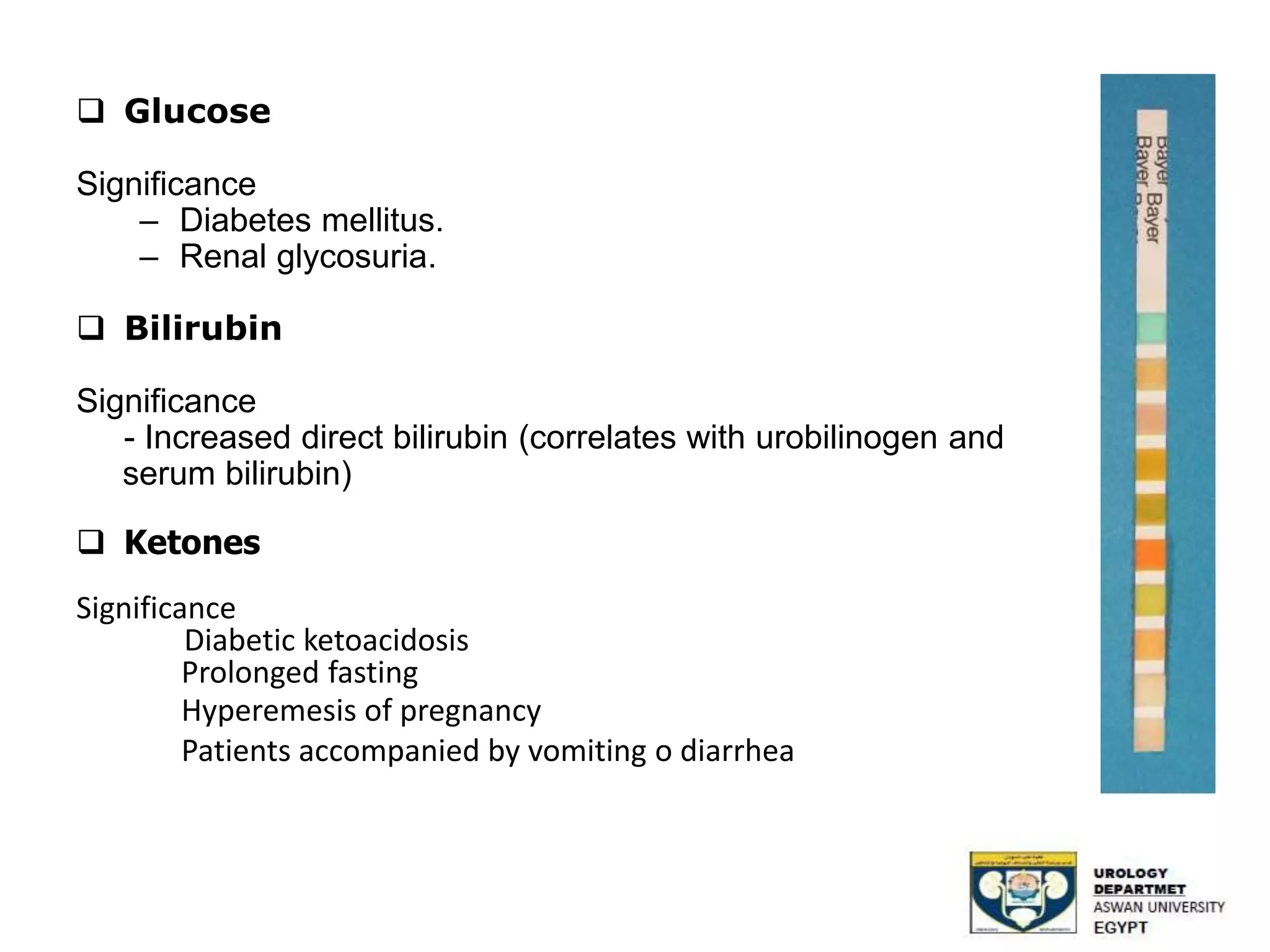
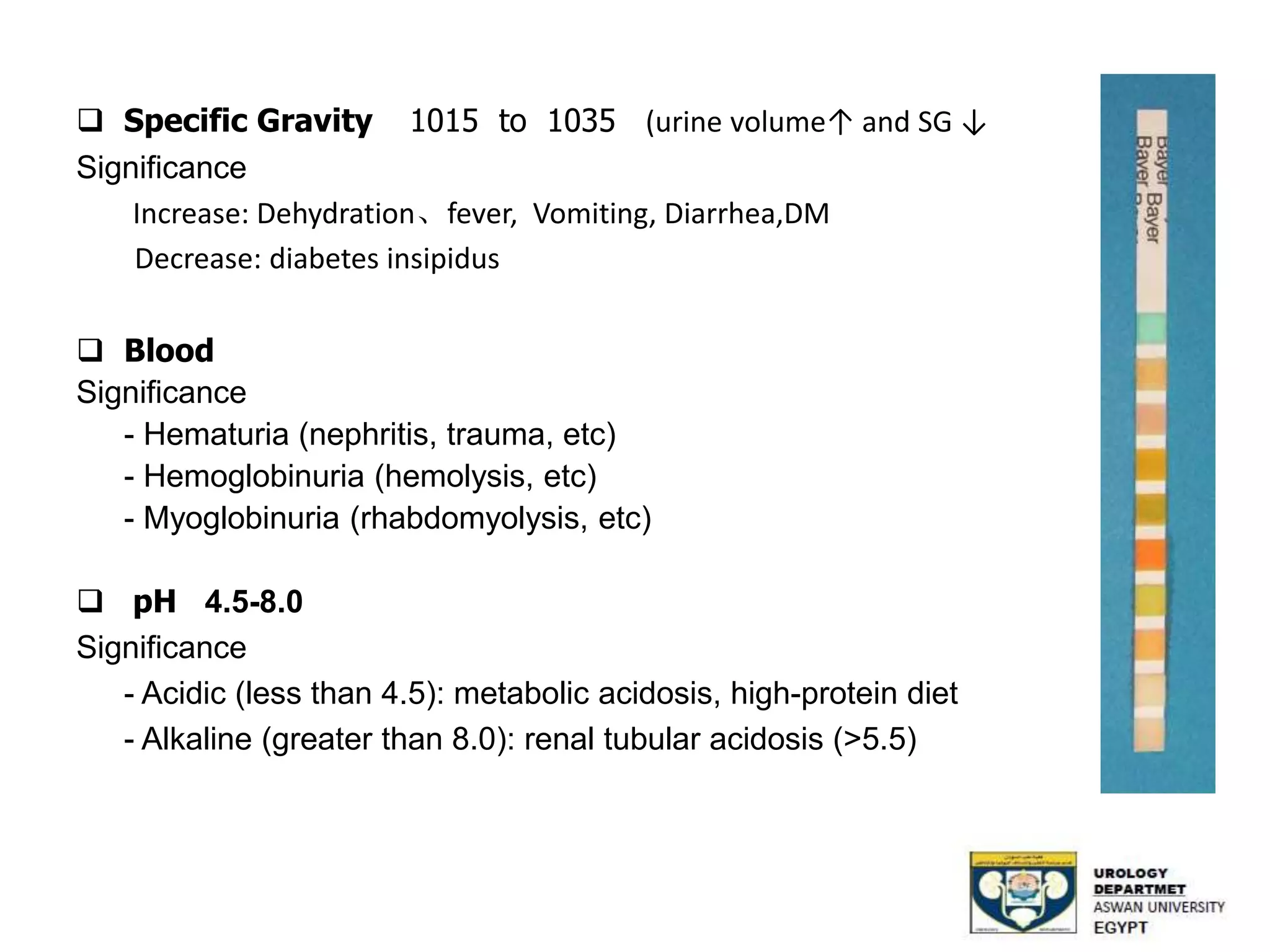
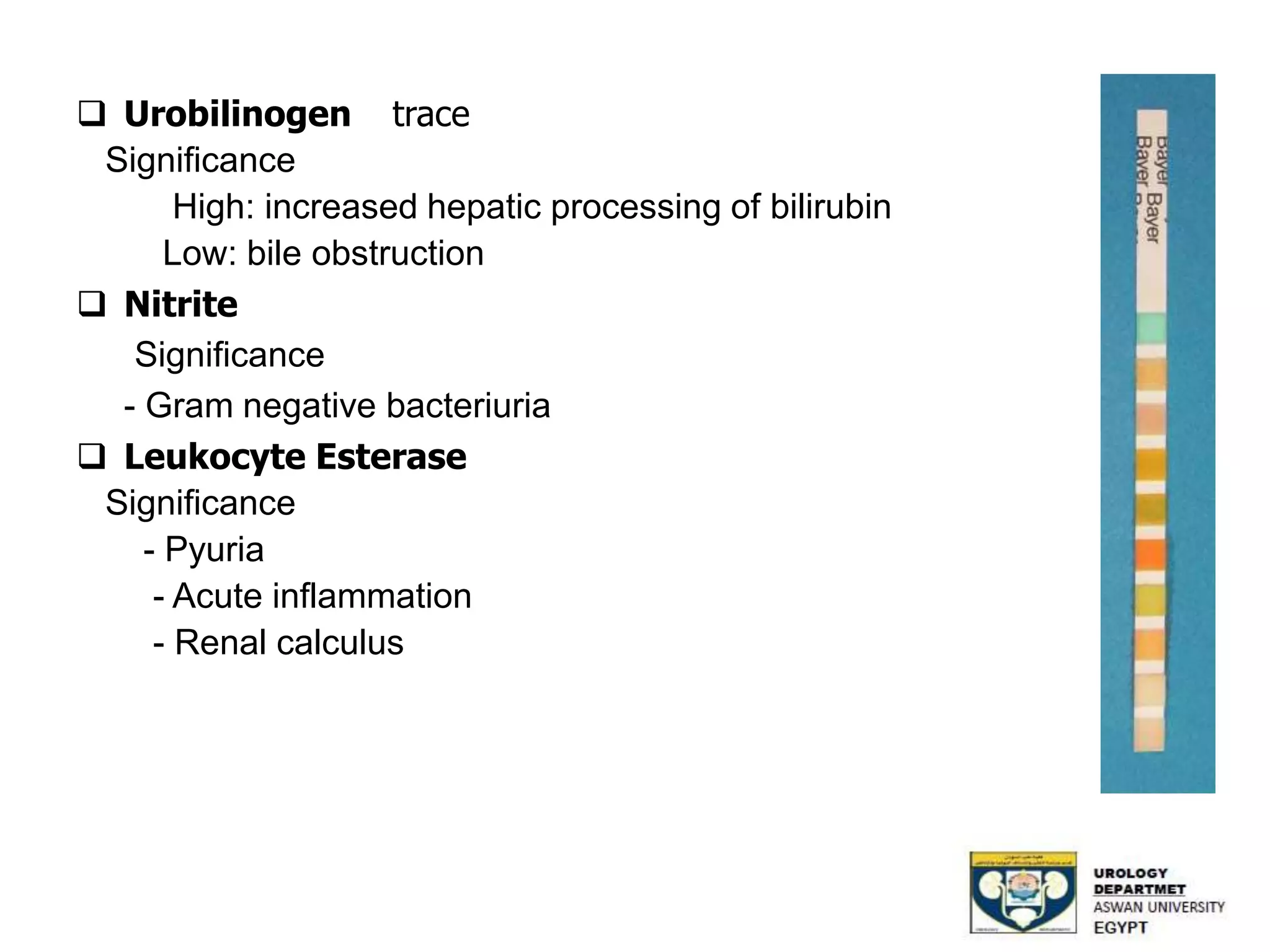
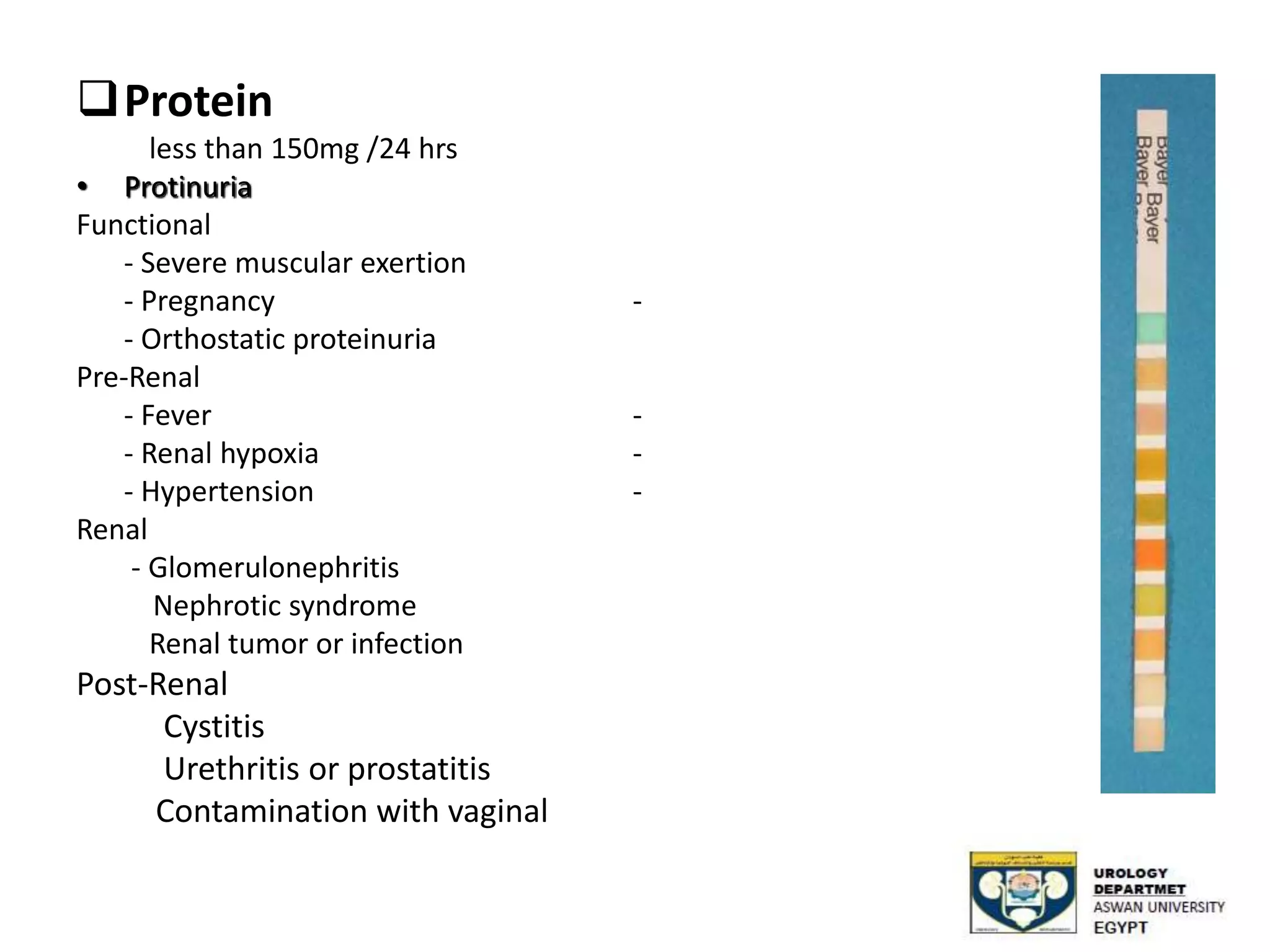
Importance of chemical analysis through dipstick tests for parameters like pH, glucose, and protein.
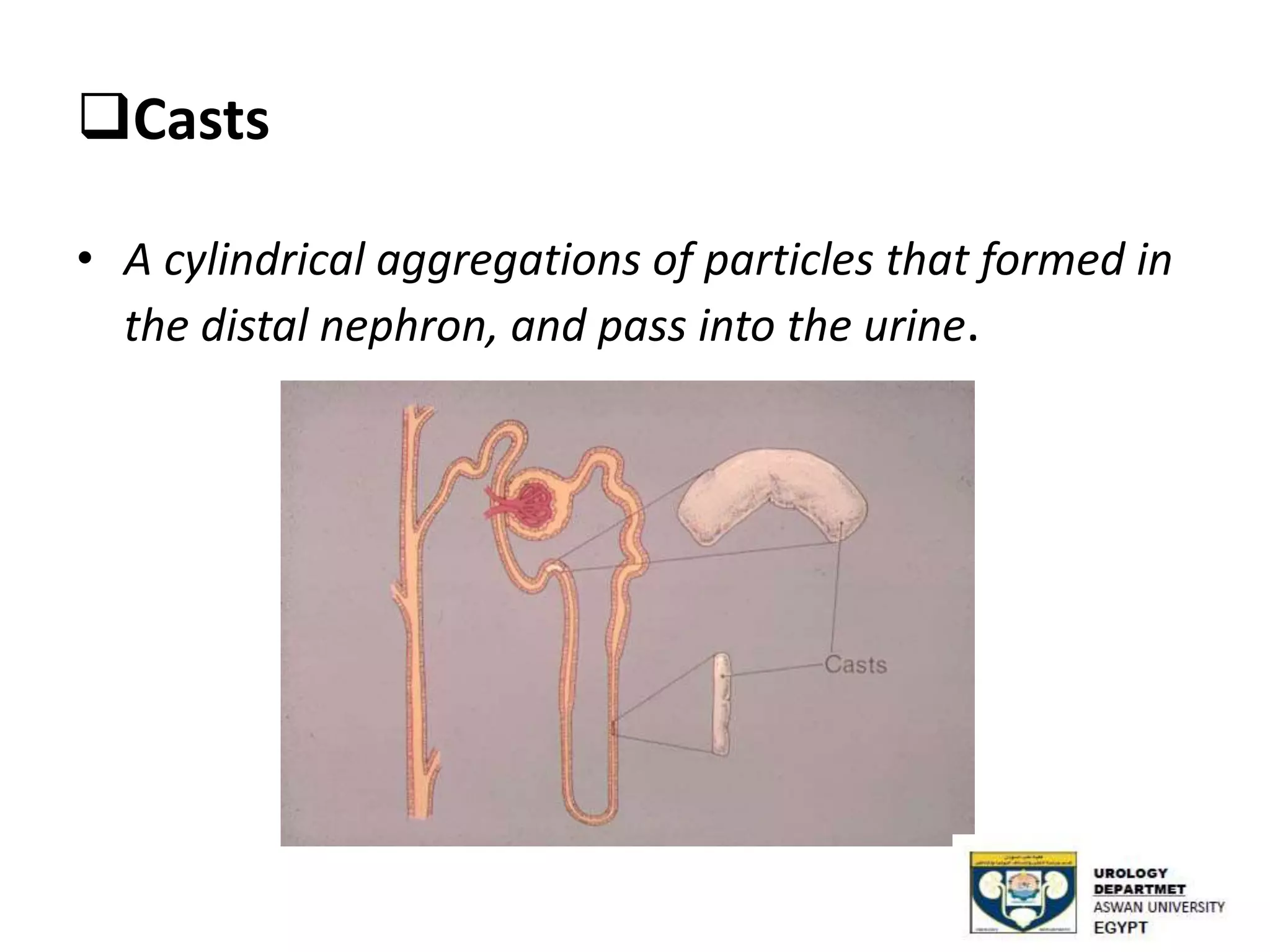
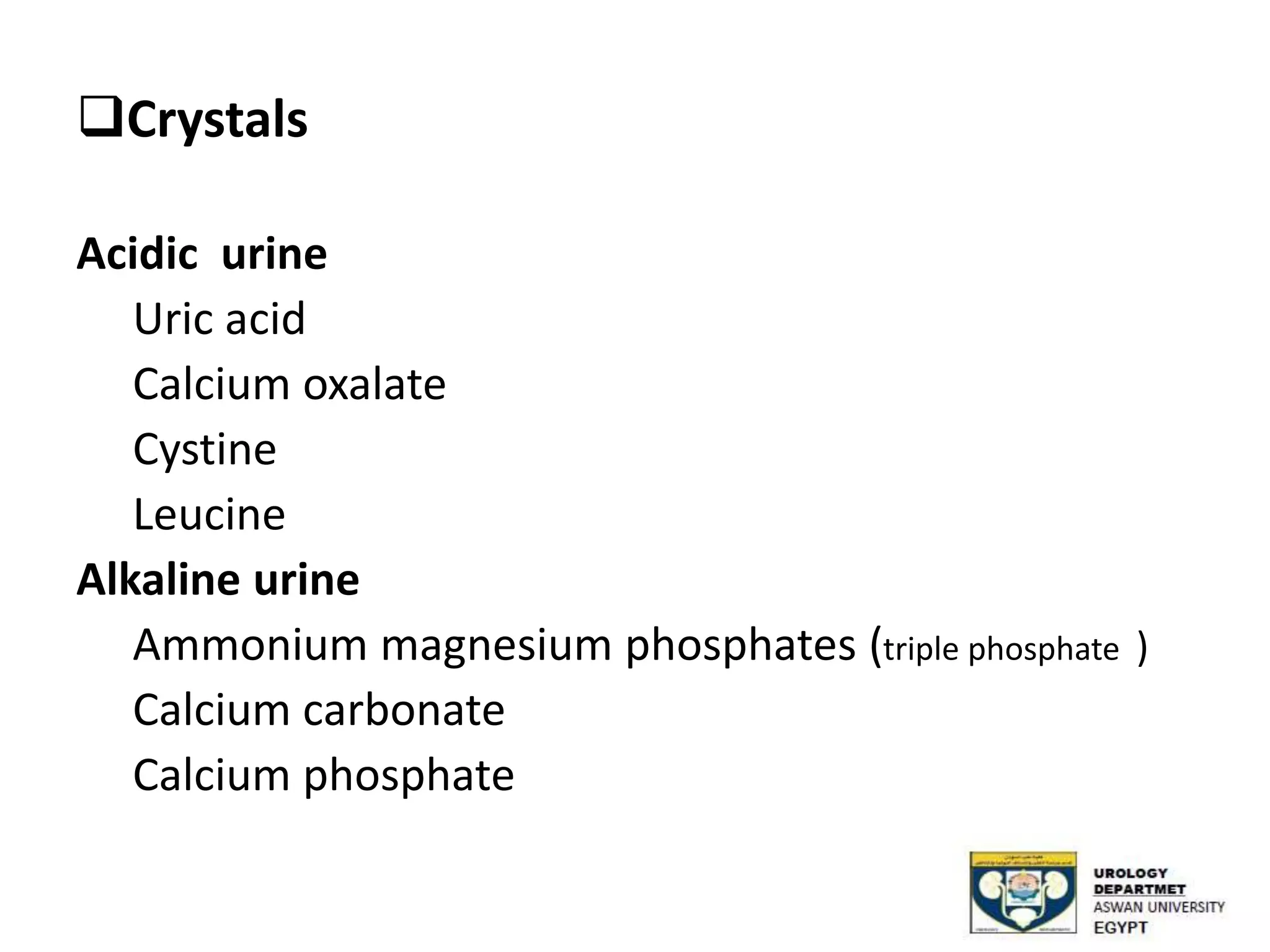
Microscopic examination of urine sediment focusing on various components such as RBCs, WBCs, bacteria, and casts.
Normal urinary volume definitions along with classifications of polyuria, oliguria, and anuria.
Final slide with a question session and expression of gratitude.























































































