Agenda of Discussion
•Pathophysiology
• Evaluation
• Imaging modalities
• Management
• Stone In Special Situation
-Children
-Pregnancy
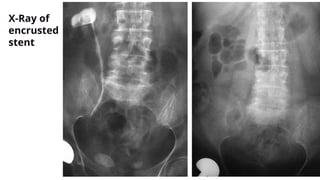
-Forgotten Encrusted Double-J Stent
3.
Pre-test
1. Metabolic changesassociated with pregnancy that are relevant to
urolithiasis include all of the following except-
a. Absorptive hypercalciuria
b. Hypercalcemia
c. Hyperuricosuria
d. Increased Magnesium excretion
4.
Pre-test
1. Metabolic changesassociated with pregnancy that are relevant to
urolithiasis include all of the following except-
a. Absorptive hypercalciuria
b. Hypercalcemia
c. Hyperuricosuria
d. Increased Magnesium excretion
5.
2. What isthe preferred initial diagnostic study for suspected
urolithiasis in pregnanacy-
a. X-Ray KUB
b. USG KUB
c. Non Contrast CT Urogram
d. MRI
Pre-test
6.
2. What isthe preferred initial diagnostic study for suspected
urolithiasis in pregnanacy-
a. X-Ray KUB
b. USG KUB
c. Non Contrast CT Urogram
d. MRI
Pre-test
7.
3. All ofthe following treatments of an obstructing ureteral calculus in
a pregnant women are EXCEPT-
a. Uretroscopy
b. Placement of a Double-J Stent
c. Placement of a nephrostomy drain
d. Shockwave Lithotripsy
Pre-test
8.
3. All ofthe following treatments of an obstructing ureteral calculus in
a pregnant women are EXCEPT-
a. Uretroscopy
b. Placement of a Double-J Stent
c. Placement of a nephrostomy drain
d. Shockwave Lithotripsy
Pre-test
9.
4. Risk factorsfor colon injury during PCNL include all of the following
except-
a. Horseshoe kidney
b. Kyphoscoliosis
c. Previous jejunoileal bypass for obesity
d. Upper pole puncture
Pre-test
10.
4. Risk factorsfor colon injury during PCNL include all of the following
except-
a. Horseshoe kidney
b. Kyphoscoliosis
c. Previous jejunoileal bypass for obesity
d. Upper pole puncture
Pre-test
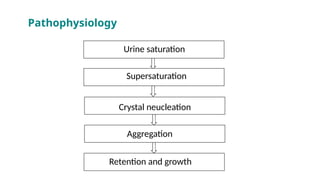
• Urine mustbe supersaturated for stones to form.
• Supersaturation alone is not sufficient for crystallization to
occur in urine because of the presence of urinary inhibitors.
• Nephrocalcin, uropontin, and Tamm-Horsfall proteins are
important inhibitors of crystal nucleation, growth, or
aggregation.
• Urinary calcium and oxalate contribute equally to urinary
saturation of calcium oxalate.
Key Points: Physicochemistry And Pathogenesis
13.
• Common calciumstones may originate from subepithelial
plaques composed of calcium apatite that serve as an anchor
on which calcium oxalate stones can grow.
• The noncrystalline component of stones is matrix, which is
composed of a combination of mucoproteins, proteins,
carbohydrates, and urinary inhibitors.
Key Points: Physicochemistry And
Pathogenesis (Cotd.)
14.
Classification of Stones
Stonesize
Stone size is usually given in one or two dimensions, and stratified into those
measuring up to 5, 5-10, 10-20, and > 20 mm in largest diameter.
Stone location
Stones can be classified according to anatomical position: upper, middle, or
lower calyx; renal pelvis; upper, middle, or distal ureter; and urinary bladder.
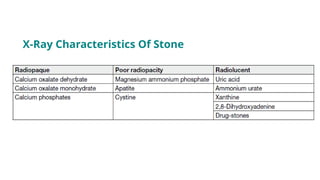
X-ray characteristics
Stones can be classified according to plain X-ray appearance [kidney-ureter-
bladder (KUB) radiography]
Kim, S.C., Burns, E.K., Lingeman, J.E. et al. Cystine calculi: correlation of CT-visible structure, CT number,
and stone morphology with fragmentation by shock wave lithotripsy. Urol Res 35, 319–324 (2007).
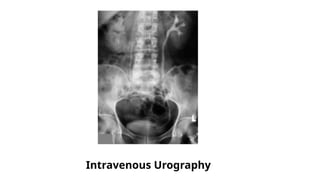
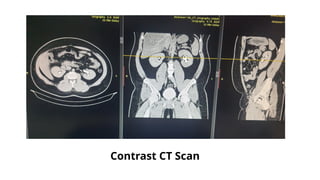
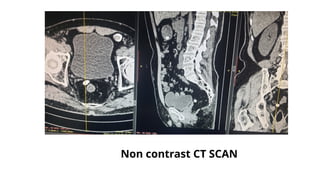
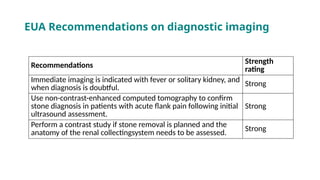
EUA Recommendations ondiagnostic imaging
Recommendations Strength
rating
Immediate imaging is indicated with fever or solitary kidney, and
when diagnosis is doubtful.
Strong
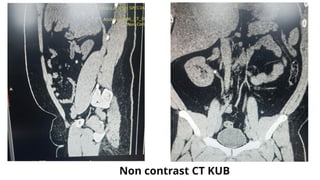
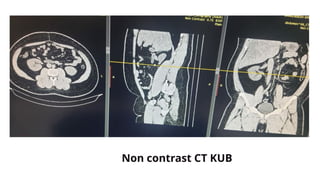
Use non-contrast-enhanced computed tomography to confirm
stone diagnosis in patients with acute flank pain following initial
ultrasound assessment.
Strong
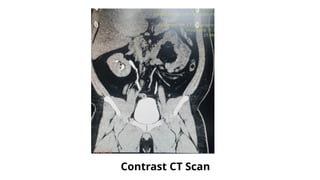
Perform a contrast study if stone removal is planned and the
anatomy of the renal collectingsystem needs to be assessed.
Strong
30.
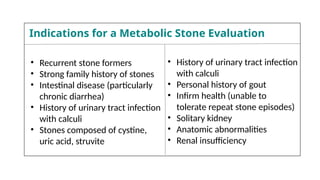
• Recurrent stoneformers
• Strong family history of stones
• Intestinal disease (particularly
chronic diarrhea)
• History of urinary tract infection
with calculi
• Stones composed of cystine,
uric acid, struvite
• History of urinary tract infection
with calculi
• Personal history of gout
• Infirm health (unable to
tolerate repeat stone episodes)
• Solitary kidney
• Anatomic abnormalities
• Renal insufficiency
Indications for a Metabolic Stone Evaluation
31.
Management of Urolithiasis
•The treatment of urolithiasis is based on many parameters
and is individualised for each patient.
• Parameters such as the size, number, location, and constitution
of the stones are cornerstones for deciding the treatment.
• In addition, the morphology, shape, volume, mobility, and hardness
of the stone should be considered.
• Finally, the anatomy and compliance of the entire pelvic-calyceal
system should be assessed for each patient.
32.
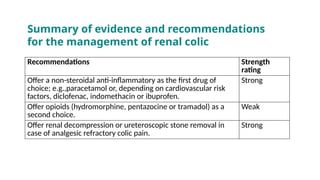
Recommendations Strength
rating
Offer anon-steroidal anti-inflammatory as the first drug of
choice; e.g.,paracetamol or, depending on cardiovascular risk
factors, diclofenac, indomethacin or ibuprofen.
Strong
Offer opioids (hydromorphine, pentazocine or tramadol) as a
second choice.
Weak
Offer renal decompression or ureteroscopic stone removal in
case of analgesic refractory colic pain.
Strong
Summary of evidence and recommendations
for the management of renal colic
33.
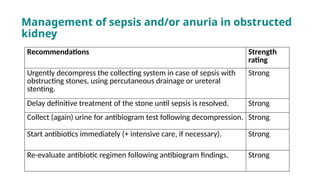
Management of sepsisand/or anuria in obstructed
kidney
Recommendations Strength
rating
Urgently decompress the collecting system in case of sepsis with
obstructing stones, using percutaneous drainage or ureteral
stenting.
Strong
Delay definitive treatment of the stone until sepsis is resolved. Strong
Collect (again) urine for antibiogram test following decompression. Strong
Start antibiotics immediately (+ intensive care, if necessary). Strong
Re-evaluate antibiotic regimen following antibiogram findings. Strong
34.
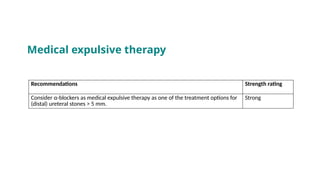
Recommendations Strength rating
Considerα-blockers as medical expulsive therapy as one of the treatment options for
(distal) ureteral stones > 5 mm.
Strong
Medical expulsive therapy
35.
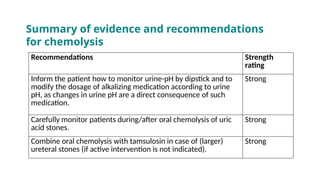
Summary of evidenceand recommendations
for chemolysis
Recommendations Strength
rating
Inform the patient how to monitor urine-pH by dipstick and to
modify the dosage of alkalizing medication according to urine
pH, as changes in urine pH are a direct consequence of such
medication.
Strong
Carefully monitor patients during/after oral chemolysis of uric
acid stones.
Strong
Combine oral chemolysis with tamsulosin in case of (larger)
ureteral stones (if active intervention is not indicated).
Strong
36.
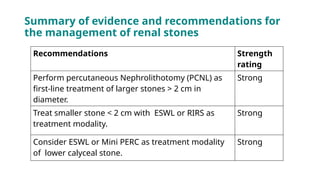
Summary of evidenceand recommendations for
the management of renal stones
Recommendations Strength
rating
Perform percutaneous Nephrolithotomy (PCNL) as
first-line treatment of larger stones > 2 cm in
diameter.
Strong
Treat smaller stone < 2 cm with ESWL or RIRS as
treatment modality.
Strong
Consider ESWL or Mini PERC as treatment modality
of lower calyceal stone.
Strong
37.
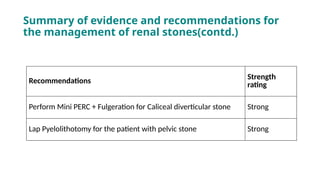
Summary of evidenceand recommendations for
the management of renal stones(contd.)
Recommendations
Strength
rating
Perform Mini PERC + Fulgeration for Caliceal diverticular stone Strong
Lap Pyelolithotomy for the patient with pelvic stone Strong
38.
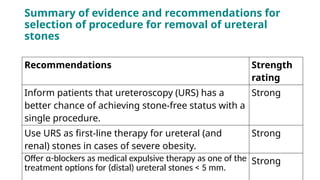
Summary of evidenceand recommendations for
selection of procedure for removal of ureteral
stones
Recommendations Strength
rating
Inform patients that ureteroscopy (URS) has a
better chance of achieving stone-free status with a
single procedure.
Strong
Use URS as first-line therapy for ureteral (and
renal) stones in cases of severe obesity.
Strong
Offer α-blockers as medical expulsive therapy as one of the
treatment options for (distal) ureteral stones < 5 mm.
Strong
39.
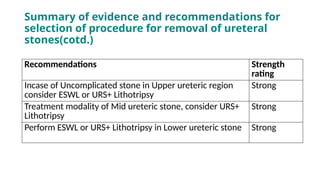
Summary of evidenceand recommendations for
selection of procedure for removal of ureteral
stones(cotd.)
Recommendations Strength
rating
Incase of Uncomplicated stone in Upper ureteric region
consider ESWL or URS+ Lithotripsy
Strong
Treatment modality of Mid ureteric stone, consider URS+
Lithotripsy
Strong
Perform ESWL or URS+ Lithotripsy in Lower ureteric stone Strong
40.
Recommendations Strength
rating
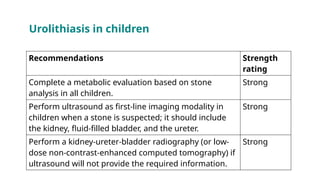
Complete ametabolic evaluation based on stone
analysis in all children.
Strong
Perform ultrasound as first-line imaging modality in
children when a stone is suspected; it should include
the kidney, fluid-filled bladder, and the ureter.
Strong
Perform a kidney-ureter-bladder radiography (or low-
dose non-contrast-enhanced computed tomography) if
ultrasound will not provide the required information.
Strong
Urolithiasis in children
41.
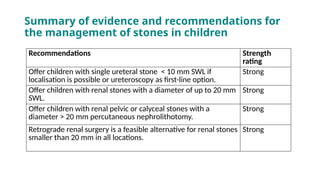
Summary of evidenceand recommendations for
the management of stones in children
Recommendations Strength
rating
Offer children with single ureteral stone < 10 mm SWL if
localisation is possible or ureteroscopy as first-line option.
Strong
Offer children with renal stones with a diameter of up to 20 mm
SWL.
Strong
Offer children with renal pelvic or calyceal stones with a
diameter > 20 mm percutaneous nephrolithotomy.
Strong
Retrograde renal surgery is a feasible alternative for renal stones
smaller than 20 mm in all locations.
Strong
• Important physiologicchanges in the kidney occur during pregnancy
and modulate urinary stone risk factors.
• Renal blood flow increases, leading to a 30% to 50% rise in glomerular
filtration rate, which subsequently increases the filtered loads of
calcium, sodium, and uric acid
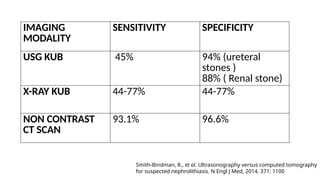
• For the detection of urolithiasis during pregnancy, low-dose CT is
associated with a higher positive predictive value (95.8%), compared
to MRI (80%) and US (77%).
Scales CD Jr, Tasian GE, Schwaderer AL, Goldfarb DS, Star RA, Kirkali Z. Urinary Stone Disease: Advancing
Knowledge, Patient Care, and Population Health. Clin J Am Soc Nephrol. 2016 Jul 7;11(7):1305-1312.
Urolithiasis in pregnancy
46.
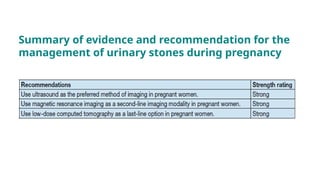
Summary of evidenceand recommendation for the
management of urinary stones during pregnancy
Aravantinos E, GravasS, Karatzas AD, Tzortzis V, Melekos M. Forgotten, encrusted ureteral stents:
a challenging problem with an endourologic solution. J Endourol. 2006 Dec;20(12):1045-9.
50.
References
• Campbell WalshWein Urology, 12th Edition. lan W. Partin & Roger R. Dmochowski & Louis R. Kavoussi &
Craig A. Peters & Alan J. Wein
• The European Association of Urology (EAU) Urolithiasis Guidelines.
http://uroweb.org/guideline/urolithiasis/.
• Aravantinos E, Gravas S, Karatzas AD, Tzortzis V, Melekos M. Forgotten, encrusted ureteral stents: a
challenging problem with an endourologic solution. J Endourol. 2006 Dec;20(12):1045-9.
• Worster, A., et al. The accuracy of noncontrast helical computed tomography versus intravenous
pyelography in the diagnosis of suspected acute urolithiasis: a meta-analysis. Ann Emerg Med,2002. 40:
280.https://pubmed.ncbi.nlm.nih.gov/12192351/
• Kim, S.C., Burns, E.K., Lingeman, J.E. et al. Cystine calculi: correlation of CT-visible structure, CT number,
and stone morphology with fragmentation by shock wave lithotripsy. Urol Res 35, 319–324 (2007).
• Smith-Bindman, R., et al. Ultrasonography versus computed tomography for suspected nephrolithiasis. N
Engl J Med, 2014. 371: 1100
• Scales CD Jr, Tasian GE, Schwaderer AL, Goldfarb DS, Star RA, Kirkali Z. Urinary Stone Disease: Advancing
• Knowledge, Patient Care, and Population Health. Clin J Am Soc Nephrol. 2016 Jul 7;11(7):1305-1312.

![Classification of Stones
Stone size
Stone size is usually given in one or two dimensions, and stratified into those
measuring up to 5, 5-10, 10-20, and > 20 mm in largest diameter.
Stone location
Stones can be classified according to anatomical position: upper, middle, or
lower calyx; renal pelvis; upper, middle, or distal ureter; and urinary bladder.
X-ray characteristics
Stones can be classified according to plain X-ray appearance [kidney-ureter-
bladder (KUB) radiography]
Kim, S.C., Burns, E.K., Lingeman, J.E. et al. Cystine calculi: correlation of CT-visible structure, CT number,
and stone morphology with fragmentation by shock wave lithotripsy. Urol Res 35, 319–324 (2007).](https://image.slidesharecdn.com/urolithiasis-250724201458-ed5435dc/85/A-Presentation-on-urinary-stone-disease-pptx-14-320.jpg)