Download to read offline
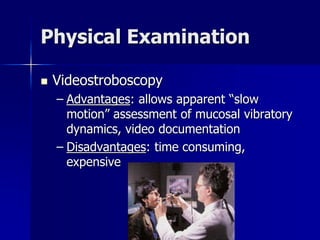


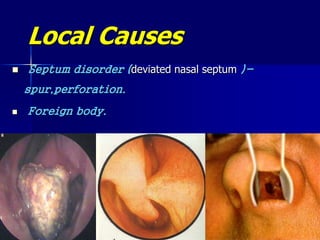
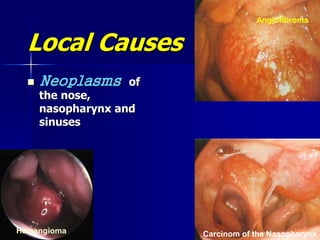



Hoarseness is a symptom of various underlying conditions, from simple inflammation to serious diseases like cancer, and it can arise from misuse, structural impairment, neurogenic issues, and psychological factors. Different examinations, including laryngoscopy, are necessary to identify the cause, while conditions like steroid inhaler laryngitis and muscle tension dysphonia require specific management strategies. Additionally, chronic pharyngitis and epistaxis are discussed, highlighting the importance of identifying local and systemic causes.






































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















