Downloaded 158 times


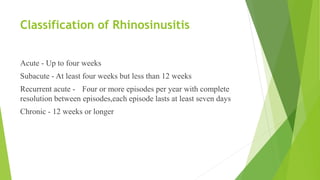
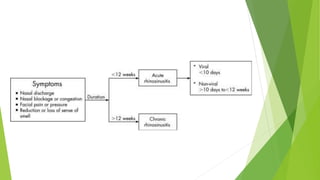




Acute rhinosinusitis is characterized by inflammation of the paranasal sinuses and nasal cavity lasting up to 4 weeks, often stemming from viral infections like the common cold. Diagnosis is primarily clinical, with symptoms including nasal discharge, blockage, and facial pain, while treatment involves antibiotics and symptom management. Complications can include serious infections, and recent studies indicate limited benefit from systemic corticosteroids in treatment efficacy.



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






