Download to read offline

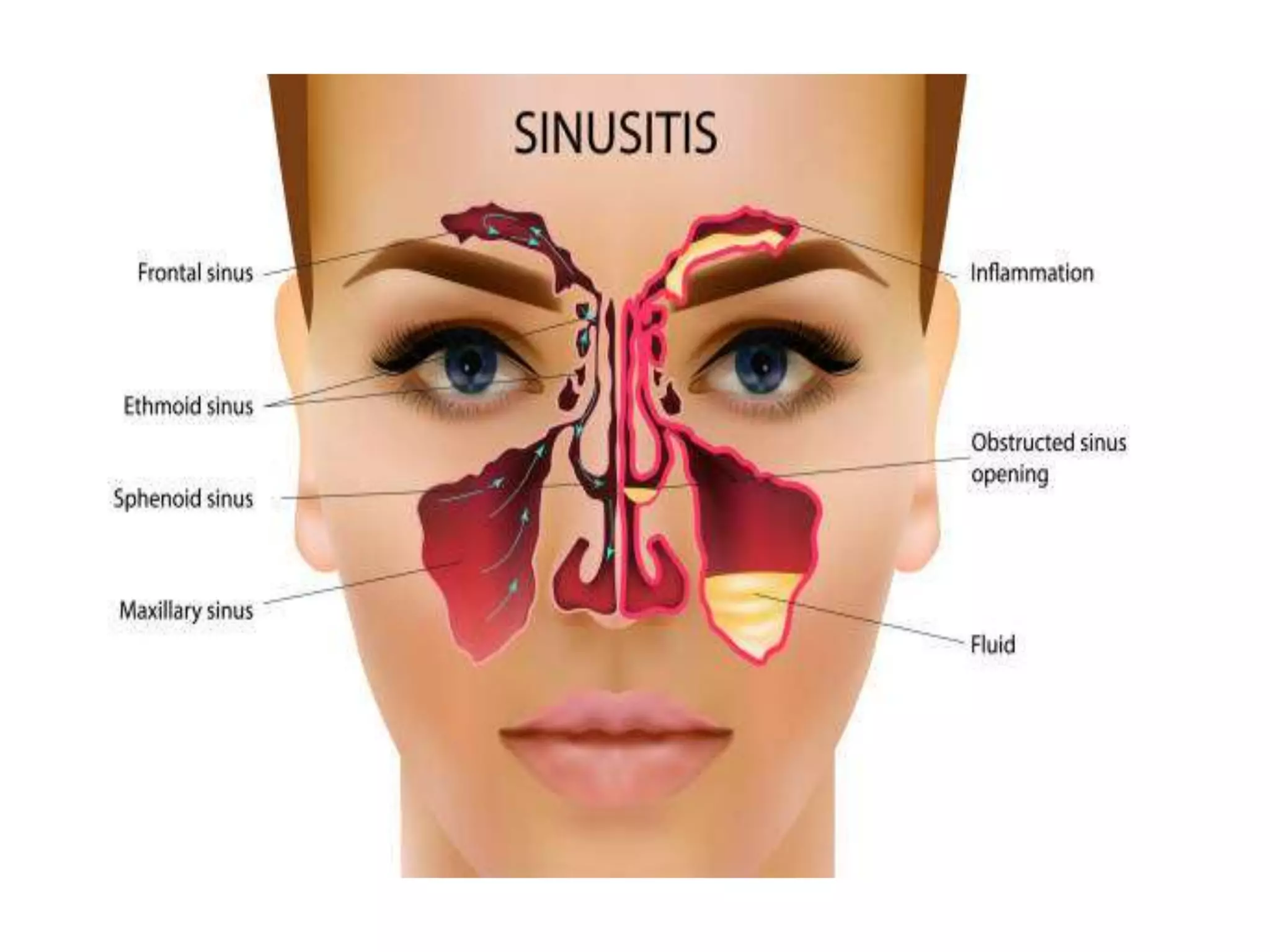
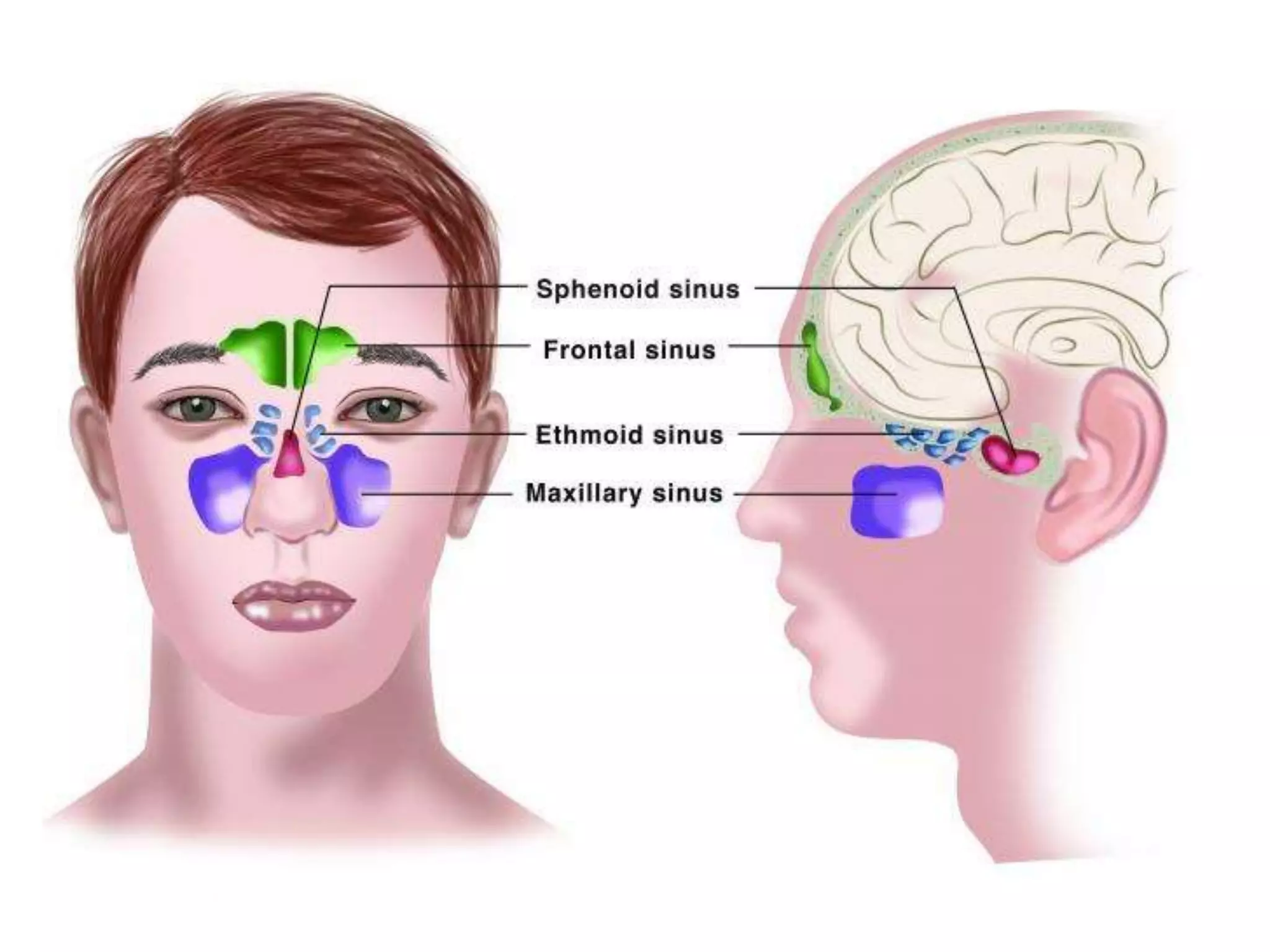










This document discusses sinusitis, including its causes, types, symptoms, and treatment. Sinusitis is an inflammation of the paranasal sinus cavities caused most commonly by viral or bacterial infections. The symptoms of acute sinusitis include nasal congestion, discharge, facial pain and fever, while chronic sinusitis involves more persistent symptoms. Common bacteria that cause acute sinusitis are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. Treatment involves antibiotics such as amoxicillin for uncomplicated cases. The document also presents a case study of a patient with suspected bacterial sinusitis and recommends amoxicillin/clavulanate treatment.























































































