Downloaded 617 times
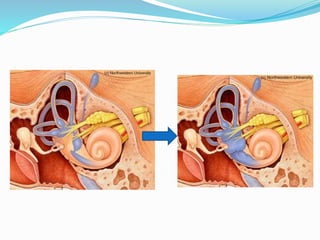
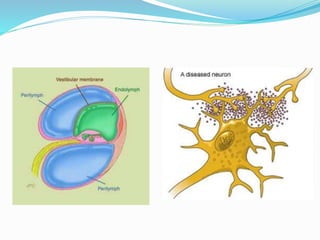
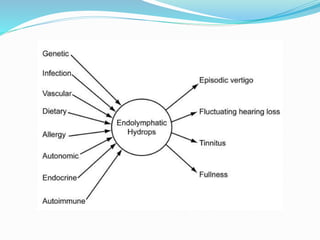
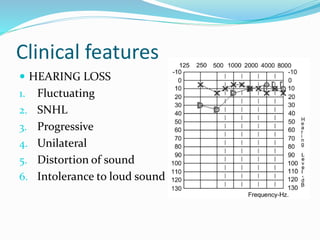

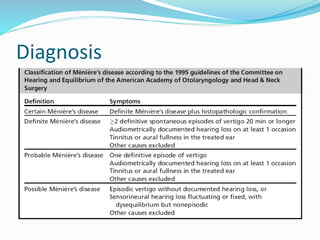
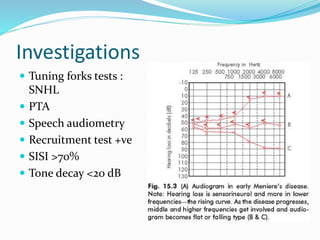
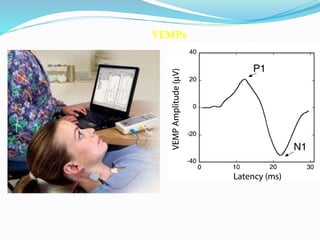
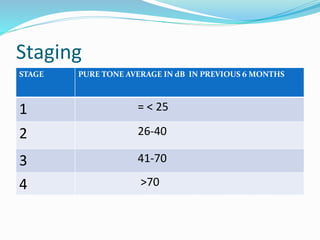
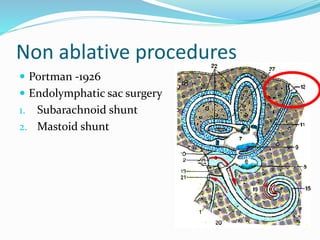

The document discusses Meniere's disease, which is a disorder of the inner ear characterized by episodes of vertigo, hearing loss, tinnitus, and a feeling of fullness. It was first described by Prosper Meniere in 1861. The pathology involves a distortion of the membranous labyrinth and endolymphatic hydrops. Symptoms include episodic vertigo, fluctuating hearing loss, tinnitus, and aural fullness. Diagnosis involves tests like caloric testing, ENG, and VEMPs. Treatments range from medical management to non-ablative procedures like endolymphatic sac surgery to ablative procedures like intratympanic gentamicin or vest










































































