Download to read offline
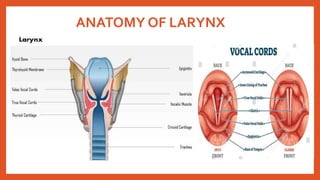
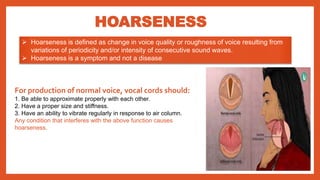
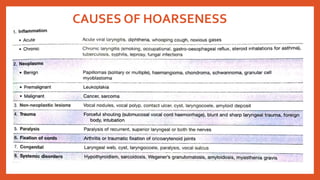
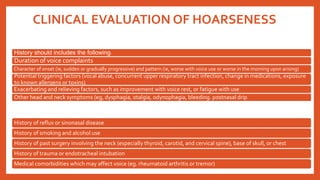
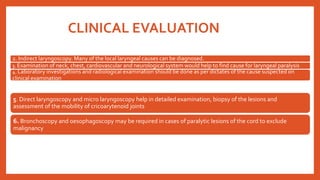


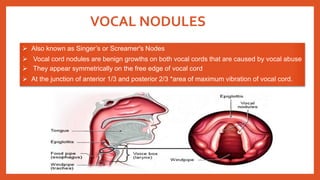



The document covers the anatomy and clinical evaluation of hoarseness, including its causes, symptoms, and treatment options. It discusses various conditions like vocal nodules, dysphonia types, vocal polyps, and vocal granulomas, alongside their management strategies. Additionally, it emphasizes the importance of proper vocal hygiene and prevention of exacerbating factors in maintaining vocal health.

















































![Down syndrome (2)[1].pptx pediatric lecture](https://cdn.slidesharecdn.com/ss_thumbnails/downsyndrome21-240709094926-fcdd02d9-thumbnail.jpg?width=640&height=640&fit=bounds)










![ABDOMINAL EXAMINATION Presentation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalexaminationpresentation1-240105120242-b6318479-thumbnail.jpg?width=640&height=640&fit=bounds)


























