Downloaded 25 times




















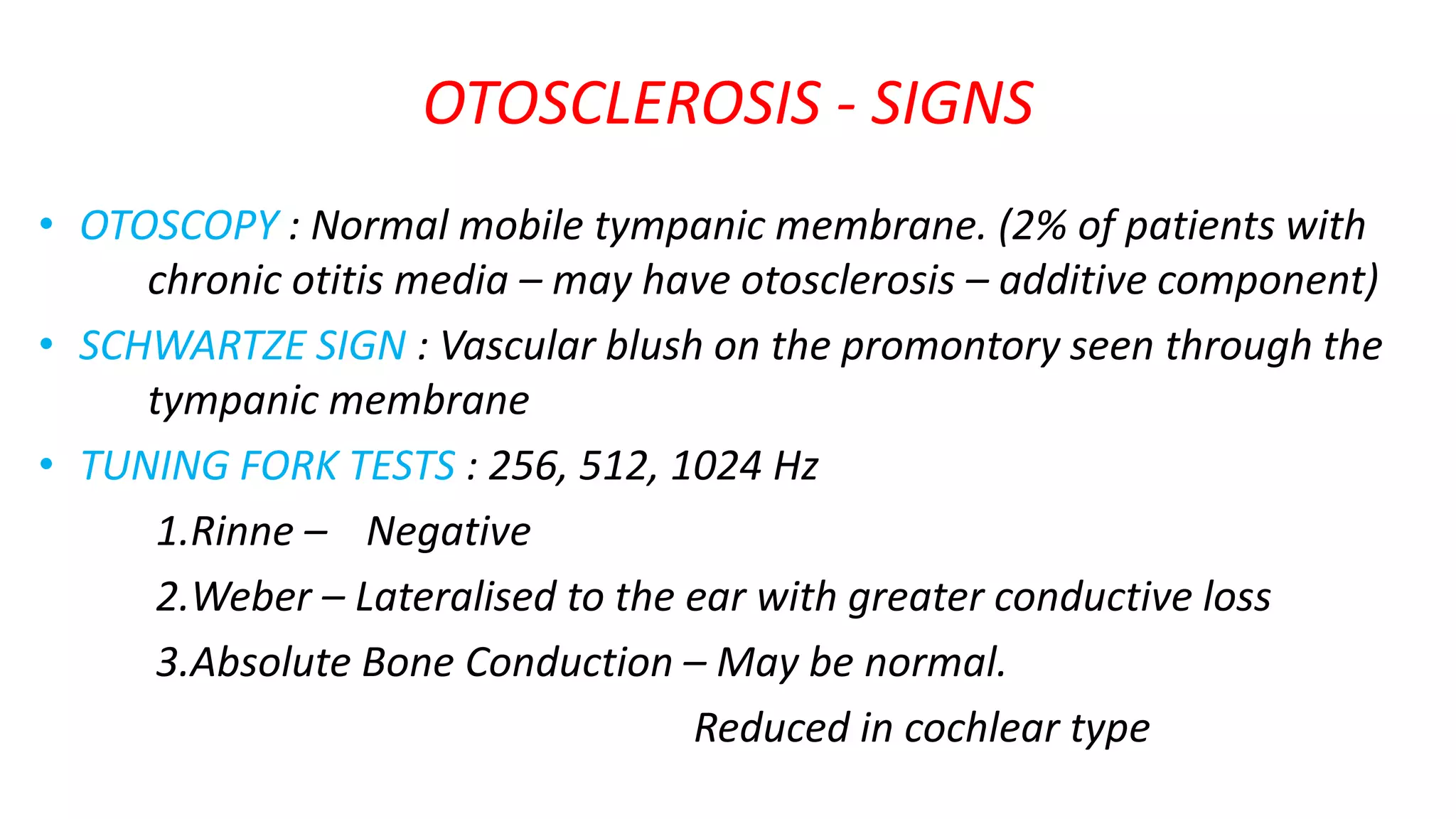








































Otosclerosis is a disease affecting the bone of the middle ear that causes conductive or mixed hearing loss. It involves abnormal bone remodeling in the inner ear capsule, most commonly at the stapes footplate, causing stapes fixation and hearing loss. Symptoms include progressive hearing loss beginning in young adults. Diagnosis is made through audiometry showing air-bone gaps and absent acoustic reflexes. Treatment involves stapedectomy or stapedotomy surgery to remove the stapes and replace it with a prosthesis to reestablish sound conduction.























































































