Downloaded 588 times



























































![• All the physiological parameters described can be used to measure anxiety
in a patient, but they all require a monitoring team, financial expenditure,
and extra time in the dental clinic. For this reason, these types of measure
are not commonly used in dental clinics
[Klingberg et al., 1995]
96](https://image.slidesharecdn.com/11-161108115029/75/Emotional-development-of-child-96-2048.jpg)






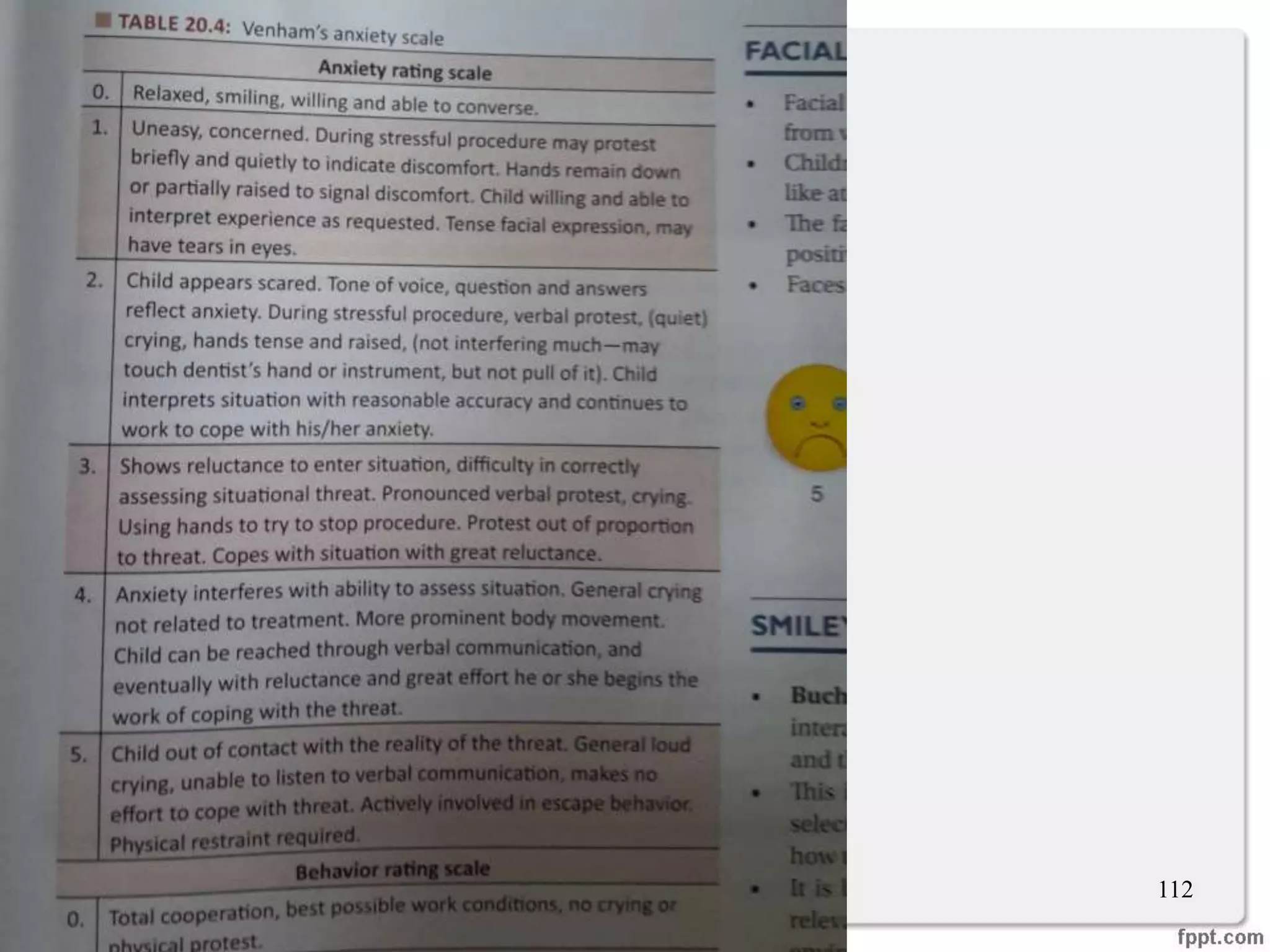
![MODIFIED CHILD DENTAL ANXIETY SCALE
"How do you feel about. . ."
104
How do you feel about. . ." relaxed-
not
worried.
very
slightly
worried,
fairly
worried,
worried
a lot,
very
worried
going to the dentist generally?
having your teeth looked at [examination]?
having your teeth scraped and polished [prophylaxis]?
having an injection in the gum [local anaesthedc]?
having a filling? 2
having a tooth taken our [extraction)?
being put to sleep to have treatment [general
anaesthesia]?
having a mixture of "gas and air" which will help you to
feel comfortable for treatment, but which cannot put you
to sleep [inhalation sedation]?
Humphris GM, Wong HM, Lee GT. Preliminary
validation and reliability of the modified child
dental anxiety scale. Psychological reports.
1998 Dec 1;83(3 suppl):1179-86.](https://image.slidesharecdn.com/11-161108115029/75/Emotional-development-of-child-104-2048.jpg)



















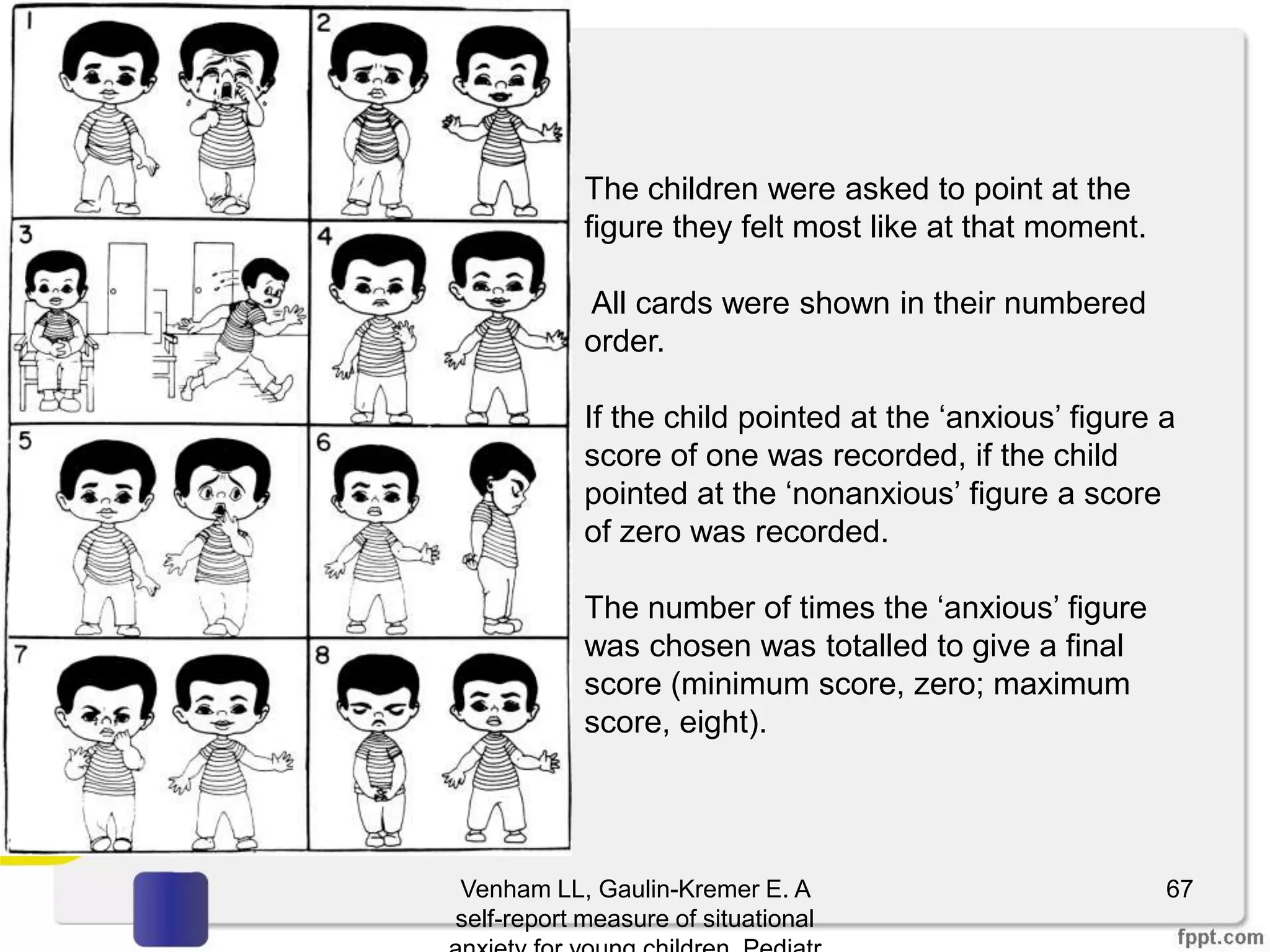
This document discusses emotional development in children. It defines emotion and explains the importance of understanding a child's emotional development when providing dental treatment. It describes the physiology of emotions, including the role of the nervous and endocrine systems. It then examines characteristics of common emotions seen in children, such as distress/crying, anger, fear, anxiety, and phobias. For each emotion, it outlines how the emotion typically presents at different developmental stages.