Downloaded 58 times


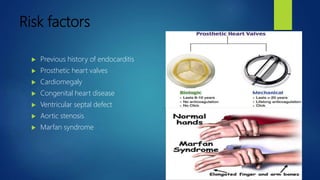

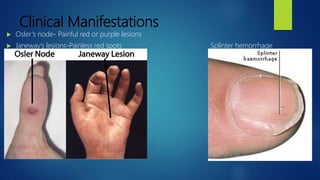


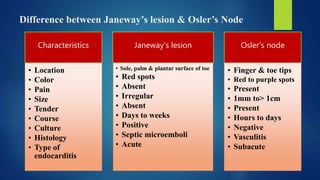






This document discusses infective endocarditis, which involves infection of the inner lining of the heart called the endocardium. It is more common in people with pre-existing heart conditions or defects. The document defines endocarditis and lists various risk factors. Common causes are bacteria like Staphylococcus aureus and Streptococcus. Symptoms may include fever, joint pain, rashes, and heart complications. Diagnosis involves blood tests, echocardiogram, and physical exam looking for signs like Osler's nodes or Janeway lesions. Treatment is usually long-term antibiotics with surgery sometimes needed to replace infected heart valves. Nursing care focuses on monitoring for complications like embolisms, decreased cardiac output, and managing






















































































