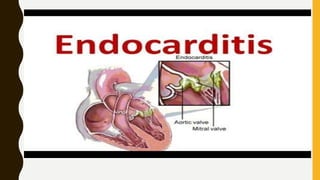



Endocarditis is inflammation of the inner lining of the heart (endocardium) that usually involves the heart valves. It is commonly caused by bacteria like Staphylococcus that enter the bloodstream through invasive procedures or wounds in the mouth, respiratory tract, GI tract, or GU tract. Risk factors include prior heart damage, dental procedures, heart surgery, and certain medical devices. Symptoms include fever, weakness, weight loss, and chest pain. Diagnosis involves blood cultures, echocardiography, and imaging tests. Treatment consists of intravenous antibiotics for 4-6 weeks to eliminate the infecting bacteria.























































































