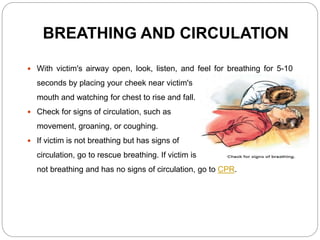
The document outlines the principles of emergency treatment and first aid, including procedures for addressing medical emergencies, such as maintaining airway, breathing, and circulation (ABCs). It details the steps involved in administering cardiopulmonary resuscitation (CPR) to victims experiencing cardiac arrest and highlights the roles and responsibilities of a first aider in preserving life, preventing further harm, and promoting recovery. Additionally, the document discusses the hospital emergency code system, particularly 'code blue,' which signifies a patient requiring immediate resuscitation.