Downloaded 98 times
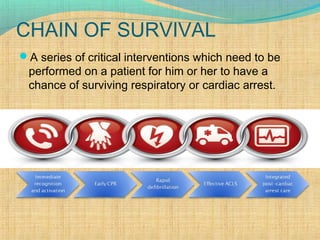
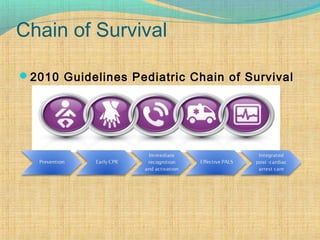
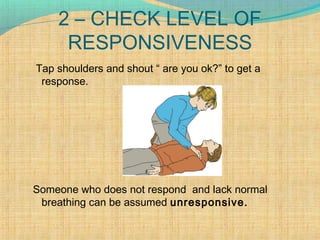
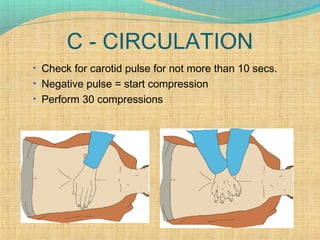
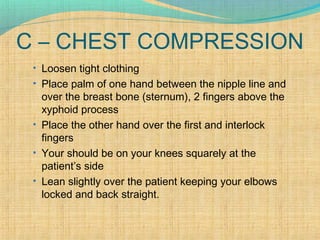
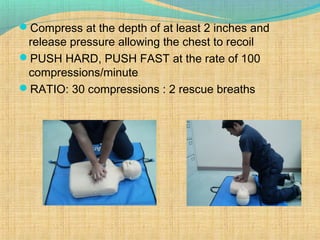
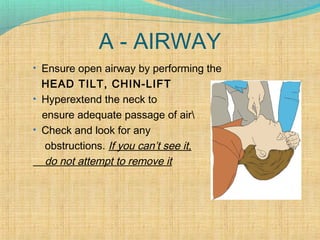
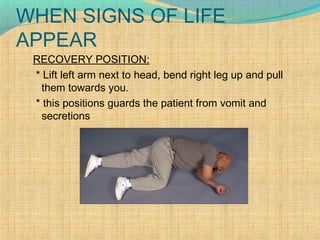
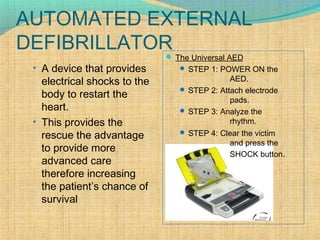
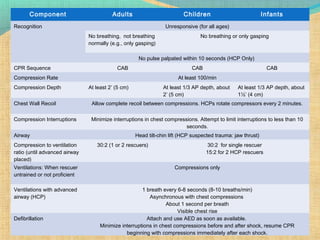


This document provides information on cardiopulmonary resuscitation (CPR) and basic life support. It discusses the components of CPR including chest compressions, rescue breathing, use of an automated external defibrillator, treatment of foreign body airway obstructions, and guidelines for performing CPR on adults, children and infants. The key steps of CPR are outlined as check for responsiveness, call for help, check breathing and pulse, then provide chest compressions and rescue breaths in a 30:2 ratio until advanced medical help arrives.






















































































