Downloaded 48 times

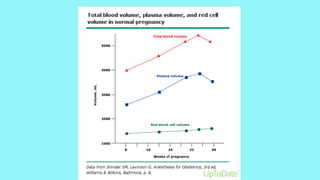
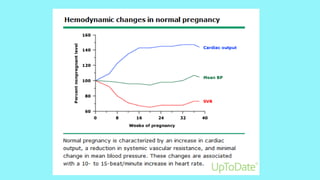

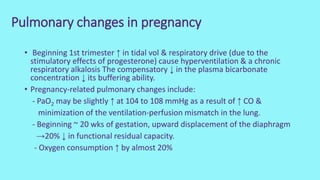
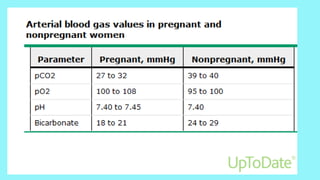
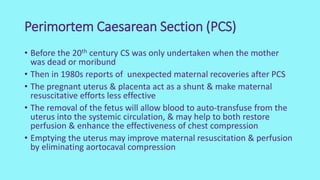
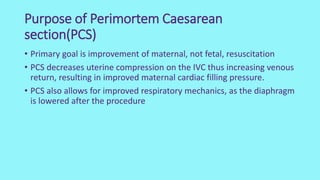
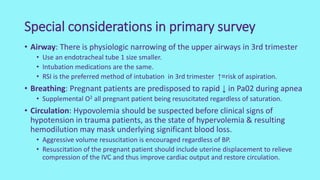

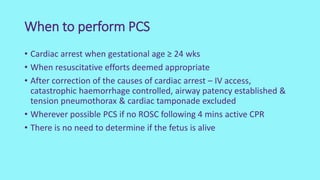
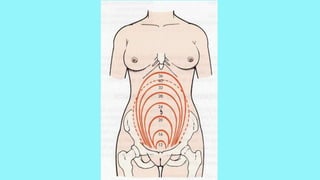

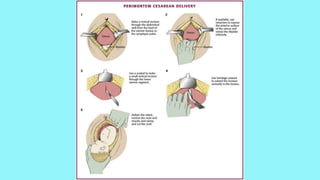


Cardiac output increases by 50% during pregnancy due to a rise in blood volume, decreased vascular resistance, and increased heart rate. Pulmonary changes include hyperventilation, upward displacement of the diaphragm reducing lung capacity by 20%, and increased oxygen consumption. Perimortem cesarean section improves maternal resuscitation by removing aortocaval compression and allowing blood to reperfuse the systemic circulation.














































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








