Downloaded 142 times
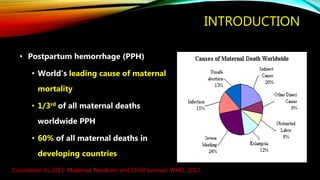
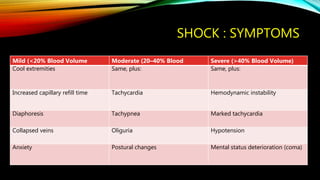
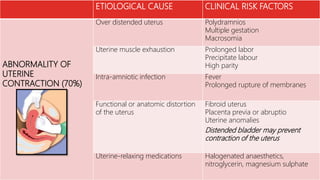


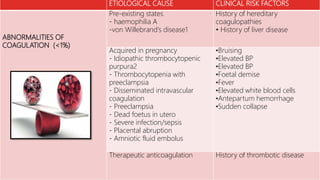



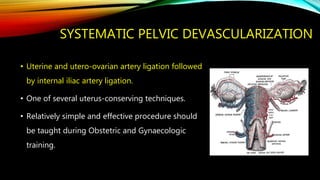


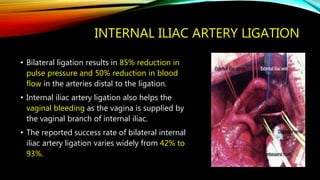


This document outlines the issues surrounding postpartum hemorrhage (PPH), its types, causes, and management strategies, stressing its significance as a leading cause of maternal mortality. It details the step-wise pelvic devascularization technique and other surgical interventions as effective methods for controlling PPH, while highlighting the importance of adequate training for healthcare providers. The document concludes that underestimating blood loss can lead to serious complications, and emphasizes the need for systematic pelvic devascularization as a vital skill in maternity care.














































![Postpartum Hemorrhage_Management_presenation[2].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pphmanagementpresenation2-250713100453-a8e3e07a-thumbnail.jpg?width=640&height=640&fit=bounds)






































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

