Downloaded 108 times
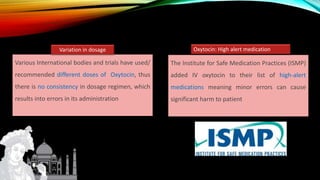
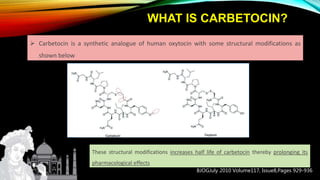
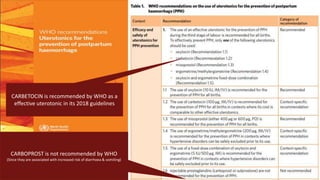
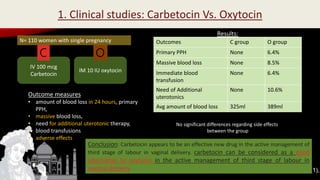
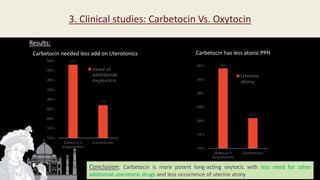



Carbetocin is a synthetic oxytocin analogue that is longer acting than oxytocin. It has a half-life of 40 minutes compared to 4-10 minutes for oxytocin. Studies show carbetocin is as effective or more effective than oxytocin in preventing postpartum hemorrhage following both vaginal and cesarean deliveries. It requires only a single dose rather than continuous infusion and does not cause uterine receptor desensitization like oxytocin. The WHO recommends carbetocin as an effective first-line uterotonic for preventing excessive bleeding after childbirth.




















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


