Downloaded 360 times
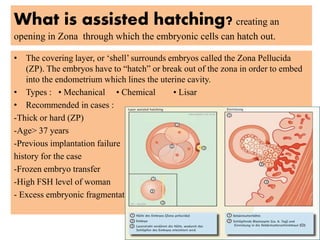
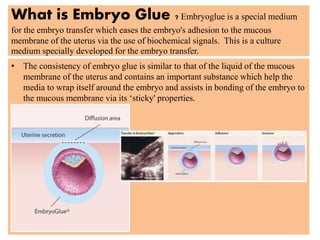
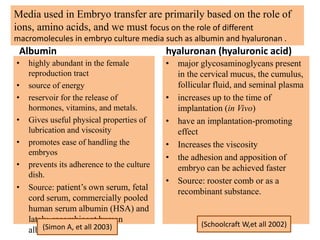
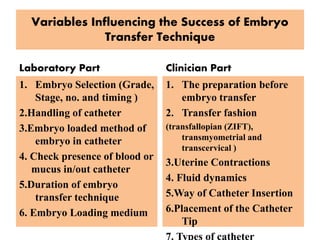
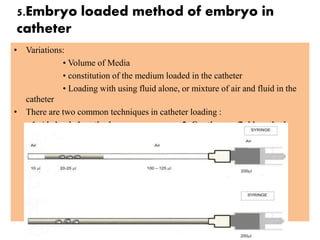
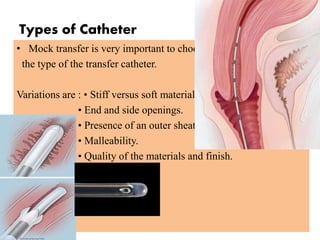


This document discusses embryo transfer as the final step of assisted reproductive technology where embryos are placed in the female uterus. It describes factors that affect embryo transfer success including implantation capacity, endometrial receptivity, and technique. The document outlines techniques for embryo transfer including assisted hatching, embryo glue, catheter type and loading, ultrasound guidance, and ensuring no blood or mucus blockage. Successful embryo transfer requires a gentle, non-traumatic procedure performed with attention to numerous technical details.





















































































