1) Embryo transfer involves placing embryos into the uterus of a female with the intent to establish a pregnancy. This can involve fresh or frozen embryos.
2) The first successful embryo transfers were conducted in rabbits in 1890 and then various livestock including sheep, cattle, pigs, and water buffalo. The first "test tube baby" was born in 1978.
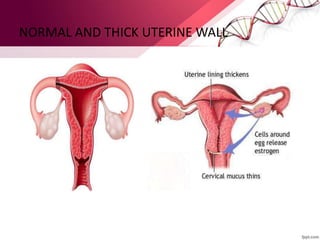
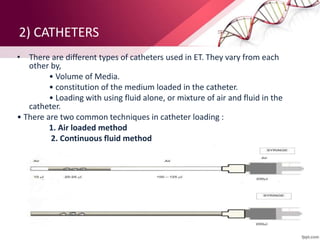
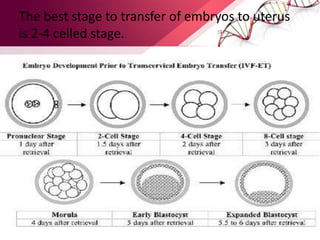
3) The embryo transfer process involves preparing the uterus, using catheters to deposit embryos, and confirming pregnancy. Embryos are typically transferred at the 2-4 cell stage. Applications include genetic improvement and conservation of endangered species.