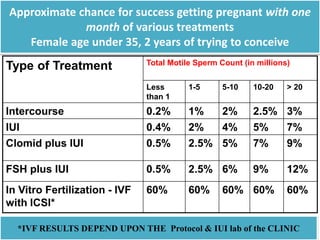
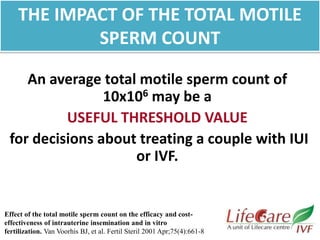
This document provides information on intrauterine insemination (IUI), including prerequisites, indications, steps, and factors affecting success rates. It summarizes that IUI is a relatively simple and inexpensive fertility treatment that involves placing sperm directly into the uterus. Success rates are affected by factors like total motile sperm count, with counts over 5 million critical. Density gradient preparation is superior to swim-up for abnormal semen. DNA fragmentation levels also impact rates. Guidelines on when to consider IVF instead of further IUI cycles include age over 37, more than 4 failed cycles, severe male factors, and certain ovarian response patterns.























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


