Downloaded 62 times
![4. Morphological assessment
Pronuclear Embryo Assessment
• Evaluation 16-18 hours following oocyte insemination (IVF) or ICSI.
• Pronucleus stadium/PN : the distribution pattern of the nucleoli (precursor
bodies) can be determined through an expensive digitalized, image-generating
method.
• Normal Fertilization: is assessed by two centrally positioned, juxtaposed PNs
with clearly defined membranes and two polar bodies.
• There are different systems for 2PN scoring:
A] Zygote-Score System (Revised zygote scoring)
B] Initial zygote scoring system
C] Ideal Features described by Tesarik and Greco](https://image.slidesharecdn.com/embryolife-160417115021/85/In-Vitro-embryo-life-12-320.jpg)
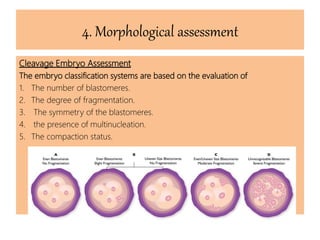


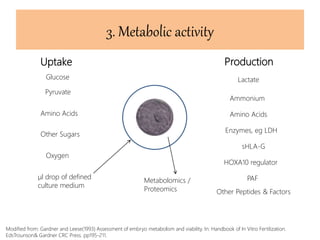
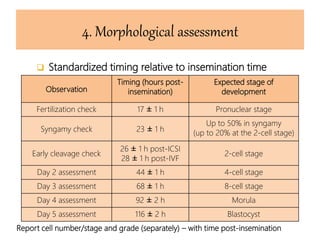
The document discusses the steps and techniques involved in assessing human embryos during pre-implantation development, focusing on criteria such as chromosomal integrity, genomic activation, metabolic activity, and morphological assessment. Key methods include preimplantation genetic diagnosis (PGD) and non-invasive techniques that evaluate embryo viability, which is crucial for successful IVF. The document also highlights the importance of specific developmental stages and assessment criteria for optimizing embryo selection and improving implantation rates.
























































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)


















