Downloaded 16 times


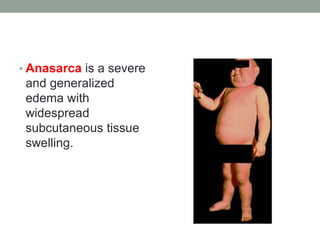
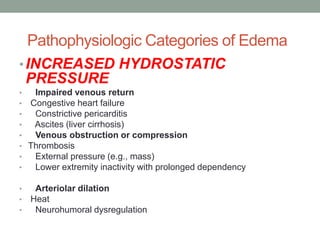

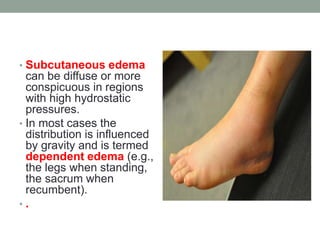

This document discusses edema, which is an abnormal accumulation of fluid in the interstitial spaces of tissues. It describes how water normally moves between blood vessels and tissues and is drained by lymphatic vessels. Edema occurs when fluid movement into tissues exceeds drainage. The main causes of edema include increased hydrostatic pressure, reduced plasma colloid osmotic pressure, lymphatic obstruction, sodium retention, and inflammation. Edema can occur in subcutaneous tissues, lungs, brain, and other body areas and cavities. The clinical consequences range from minor to life-threatening depending on the location and severity of the edema.























































































