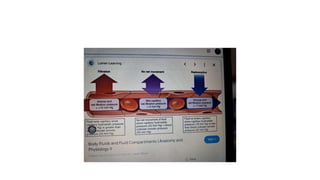
Edema is defined as the excessive accumulation of fluid in tissues, which can be generalized or localized. It is categorized into intracellular and extracellular types, with various causes including malnutrition, poor metabolism, heart failure, renal diseases, decreased plasma proteins, lymphatic obstruction, and increased endothelial permeability. The document also describes the mechanisms behind these causes and differentiates between pitting and non-pitting edema.

![• References
• 1.
• Cho S, Atwood JE. Peripheral edema. Am J Med. 2002 Nov;113(7):580-6. [PubMed]
• 2.
• Miserocchi G, Negrini D, Passi A, De Luca G. Development of lung edema: interstitial fluid
dynamics and molecular structure. News Physiol Sci. 2001 Apr;16:66-71. [PubMed]
• 3.
• Bhave G, Neilson EG. Body fluid dynamics: back to the future. J Am Soc Nephrol. 2011
Dec;22(12):2166-81. [PMC free article] [PubMed]
• 4.
• Levick JR, Michel CC. Microvascular fluid exchange and the revised Starling principle.
Cardiovasc Res. 2010 Jul 15;87(2):198-210. [PubMed]
• 5.
• Reed RK, Rubin K. Transcapillary exchange: role and importance of the interstitial fluid
pressure and the extracellular matrix. Cardiovasc Res. 2010 Jul 15;87(2):211-7. [PubMed]](https://image.slidesharecdn.com/oedematypescausespathophysiology-240606045021-f17b9d37/85/Oedema_types_causes_pathophysiology-pptx-15-320.jpg)
![• 6.
• Woodcock TE, Woodcock TM. Revised Starling equation and the glycocalyx model of transvascular fluid
exchange: an improved paradigm for prescribing intravenous fluid therapy. Br J Anaesth. 2012
Mar;108(3):384-94. [PubMed]
• 7.
• Wiig H, Schröder A, Neuhofer W, Jantsch J, Kopp C, Karlsen TV, Boschmann M, Goss J, Bry M, Rakova N,
Dahlmann A, Brenner S, Tenstad O, Nurmi H, Mervaala E, Wagner H, Beck FX, Müller DN, Kerjaschki D, Luft
FC, Harrison DG, Alitalo K, Titze J. Immune cells control skin lymphatic electrolyte homeostasis and blood
pressure. J Clin Invest. 2013 Jul;123(7):2803-15. [PMC free article] [PubMed]
• 8.
• Renkin EM. B. W. Zweifach Award lecture. Regulation of the microcirculation. Microvasc Res. 1985
Nov;30(3):251-63. [PubMed]
• 9.
• Taylor AE. Capillary fluid filtration. Starling forces and lymph flow. Circ Res. 1981 Sep;49(3):557-75.
[PubMed]
• 10.
• Crandall ED, Staub NC, Goldberg HS, Effros RM. Recent developments in pulmonary edema. Ann Intern Med.
1983 Dec;99(6):808-22. [PubMed]](https://image.slidesharecdn.com/oedematypescausespathophysiology-240606045021-f17b9d37/85/Oedema_types_causes_pathophysiology-pptx-16-320.jpg)
![• 11.
• Watkins L, Burton JA, Haber E, Cant JR, Smith FW, Barger AC. The renin-angiotensin-aldosterone system in
congestive failure in conscious dogs. J Clin Invest. 1976 Jun;57(6):1606-17. [PMC free article] [PubMed]
• 12.
• Dzau VJ, Colucci WS, Hollenberg NK, Williams GH. Relation of the renin-angiotensin-aldosterone system to clinical
state in congestive heart failure. Circulation. 1981 Mar;63(3):645-51. [PubMed]
• 13.
• Deitch EA. The management of burns. N Engl J Med. 1990 Nov 01;323(18):1249-53. [PubMed]
• 14.
• Ohlsson K, Björk P, Bergenfeldt M, Hageman R, Thompson RC. Interleukin-1 receptor antagonist reduces mortality
from endotoxin shock. Nature. 1990 Dec 06;348(6301):550-2. [PubMed]
• 15.
• Colletti LM, Remick DG, Burtch GD, Kunkel SL, Strieter RM, Campbell DA. Role of tumor necrosis factor-alpha in
the pathophysiologic alterations after hepatic ischemia/reperfusion injury in the rat. J Clin Invest. 1990
Jun;85(6):1936-43. [PMC free article] [PubMed]
• 16.
• Hommel E, Mathiesen ER, Aukland K, Parving HH. Pathophysiological aspects of edema formation in diabetic
nephropathy. Kidney Int. 1990 Dec;38(6):1187-92. [PubMed]](https://image.slidesharecdn.com/oedematypescausespathophysiology-240606045021-f17b9d37/85/Oedema_types_causes_pathophysiology-pptx-17-320.jpg)