The document defines irregular wide complex tachycardias, highlighting causes such as polymorphic ventricular tachycardia and atrial fibrillation with aberrant conduction. It details the characteristics and mechanisms of torsades de pointes, a specific form of polymorphic VT, and discusses various types including catecholaminergic polymorphic VT and bi-directional VT. Additionally, it outlines the impact of atrial fibrillation and ventricular fibrillation on heart rhythms.

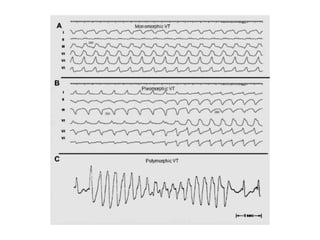
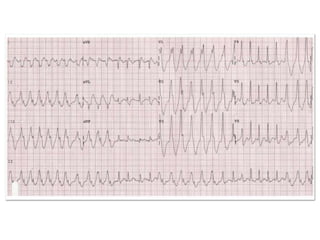
![Pleomorphic VT
• Occasionally sustained VT in alternate
morphologies[pleomorphism] such as RBBB and
LBBB. These may be gradual or abrupt.
• These changes may be gradual or abrupt, and occur
over long or short periods of time.
• Morphologies are considered to be different when
they have different patterns [RBBB or LBBB], or when
QRS deviation changes to more or equal to
45degress, even if the bundle branch block pattern is
unchanged](https://image.slidesharecdn.com/wideqrscomplexadnan-221229031442-e7a72790/85/Irregular-wide-qrs-tachycardia-8-320.jpg)
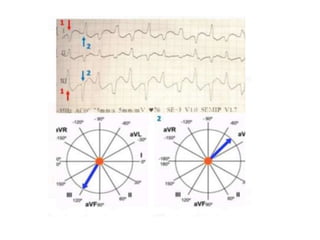
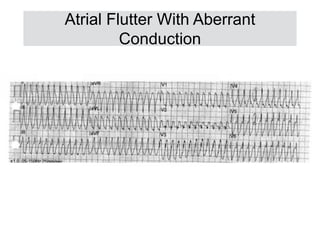
![Bi-Directional VT
• Bi- Directional tachycardias are infrequent or may be
supra ventricular [BSVT] or ventricular[DVT] origin.
• The frontal plane axis [AQRS] shows alternative
changes of approximately 180 degrees
• RR intervals are usually equal but sometimes show
bi geminal pattern.](https://image.slidesharecdn.com/wideqrscomplexadnan-221229031442-e7a72790/85/Irregular-wide-qrs-tachycardia-10-320.jpg)
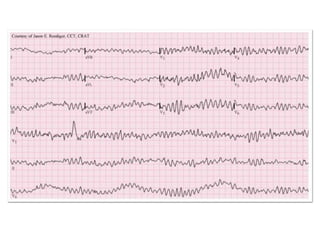
![Ventricular Fibrillation
• It is a very fast and irregular rhythm which does not
generate effective mechanical activity [>300bpm]
• It is usually triggered by a PVC and maintained as
result of repetitive micro re-entries[Similar to AF]
• ECG shows very high heart rate 300-500 beats per
min
• QRS complexes can be variable morphology and
height where QRS and ST-T are indistinguishable](https://image.slidesharecdn.com/wideqrscomplexadnan-221229031442-e7a72790/85/Irregular-wide-qrs-tachycardia-17-320.jpg)

















![Cardiccccac Arrhythmias [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cardiacarrhythmiasautosaved-241108153215-72acce97-thumbnail.jpg?width=640&height=640&fit=bounds)





























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)