The document discusses cardiac arrhythmias, particularly tachyarrhythmias, outlining their definitions, classifications, pathogenesis, and treatment approaches. It emphasizes the importance of identifying precipitating factors before pharmacological treatment, detailing various types of tachycardia, their ECG characteristics, and management recommendations. Key treatments include beta-blockers, antiarrhythmic drugs, and interventions like electrical cardioversion, depending on the specific arrhythmia type and patient condition.































































![Cardiccccac Arrhythmias [Autosaved].pptx](https://image.slidesharecdn.com/cardiacarrhythmiasautosaved-241108153215-72acce97/75/Cardiccccac-Arrhythmias-Autosaved-pptx-65-2048.jpg)
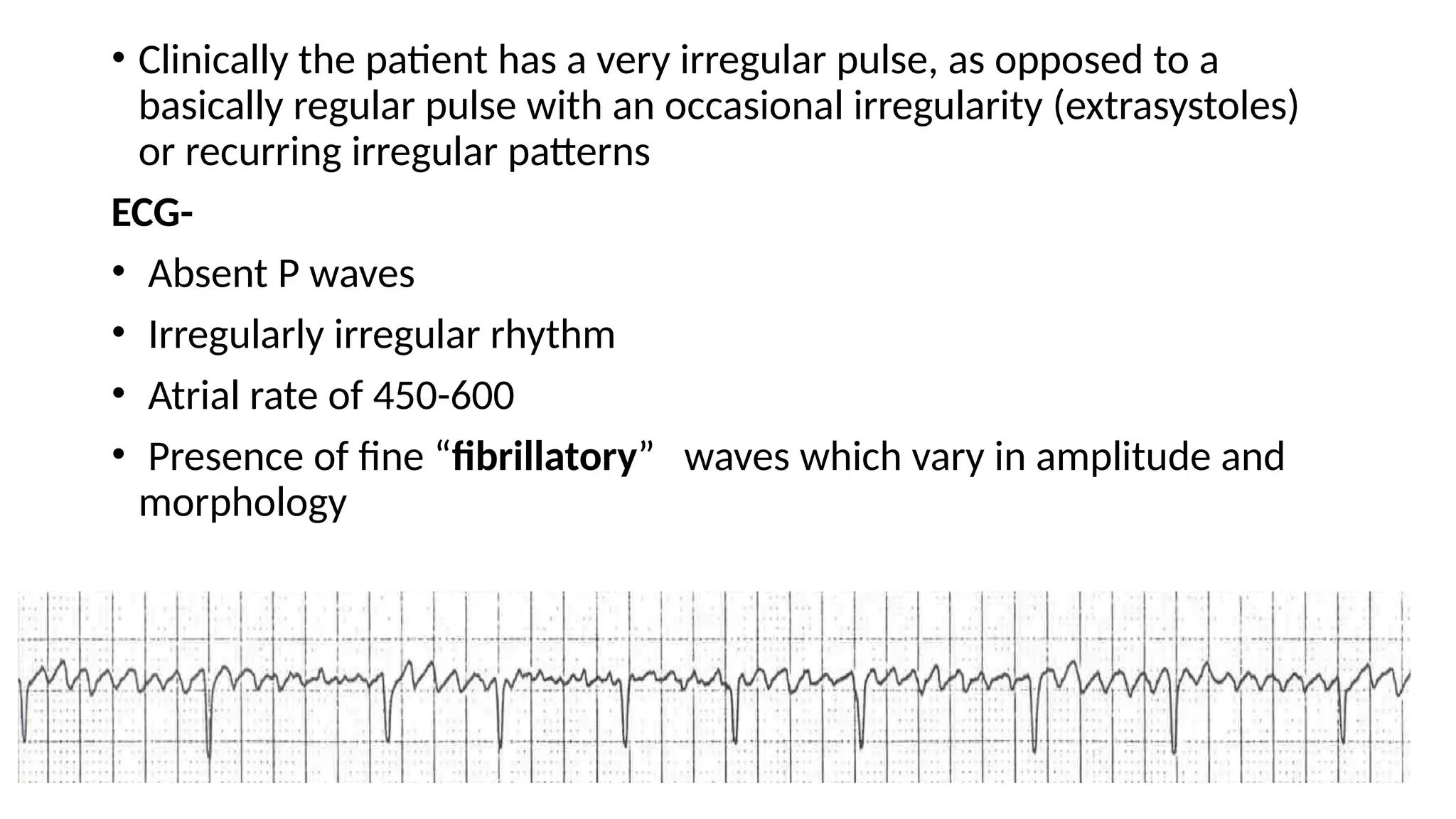
![Cardiccccac Arrhythmias [Autosaved].pptx](https://image.slidesharecdn.com/cardiacarrhythmiasautosaved-241108153215-72acce97/75/Cardiccccac-Arrhythmias-Autosaved-pptx-66-2048.jpg)
![Cardiccccac Arrhythmias [Autosaved].pptx](https://image.slidesharecdn.com/cardiacarrhythmiasautosaved-241108153215-72acce97/75/Cardiccccac-Arrhythmias-Autosaved-pptx-67-2048.jpg)
























































