Goals
To make tachycardia“less scary”
To give you an approach to tachycardia
Pearls of interpretating
3.
Case 1
• 30yo M cocaine abuser, chest pain, palpitations and SOB
• HR 162 bpm, BP 140/90mmhg, T 37 C,SO2 95%
• ECG DX?
• What is the treatment ?
4.
Cardiac Anatomy
• Sino-atrialnode (SA Node):
origin of physiologic
cardiac pacemaker
• Atrioventricular Node (AV
Node): ONLY pathway
between atria and ventricles
(AV node delay)
• Ventricles: Bundle Branches
and His-Purkinje Fibers
4
5.
Waveforms
• P Wave:Atrial
depolarization (contraction)
• PR Interval: AV node
conduction
• QRS Complex: ventricular
depolarization, conduction
through the His-Purkinje
system of the ventricles
(contraction)
• T Wave: ventricular
repolarization
6.
Normal Intervals
• PR
–0.20 sec (less than one large
box)
• QRS
– 0.08 – 0.10 sec (1-2 small
boxes)
• QT
– 450 ms in men, 460 ms in
women
– Based on sex / heart rate
– Half the R-R interval with
normal HR
7.
What am Ilooking for in the ECG?
7
Stepwise Approach to the Evaluation of Every ECG!!!
1. Ventricular RATE: Fast (>100 beats/min), slow (<60
beats/min)
2. RHYTHM: Is it sinus?? P wave before each QRS
complex?
3. RHYTHM: Regular, irregular,
regular with occasional irregularities?
4. PR, QRS intervals: PR prolonged? QRS prolonged (>0.12
sec), or normal?
5. ST segments: Dx of Ischemia or Infarction
6. T wave changes: peaked, upright, inverted, biphasic
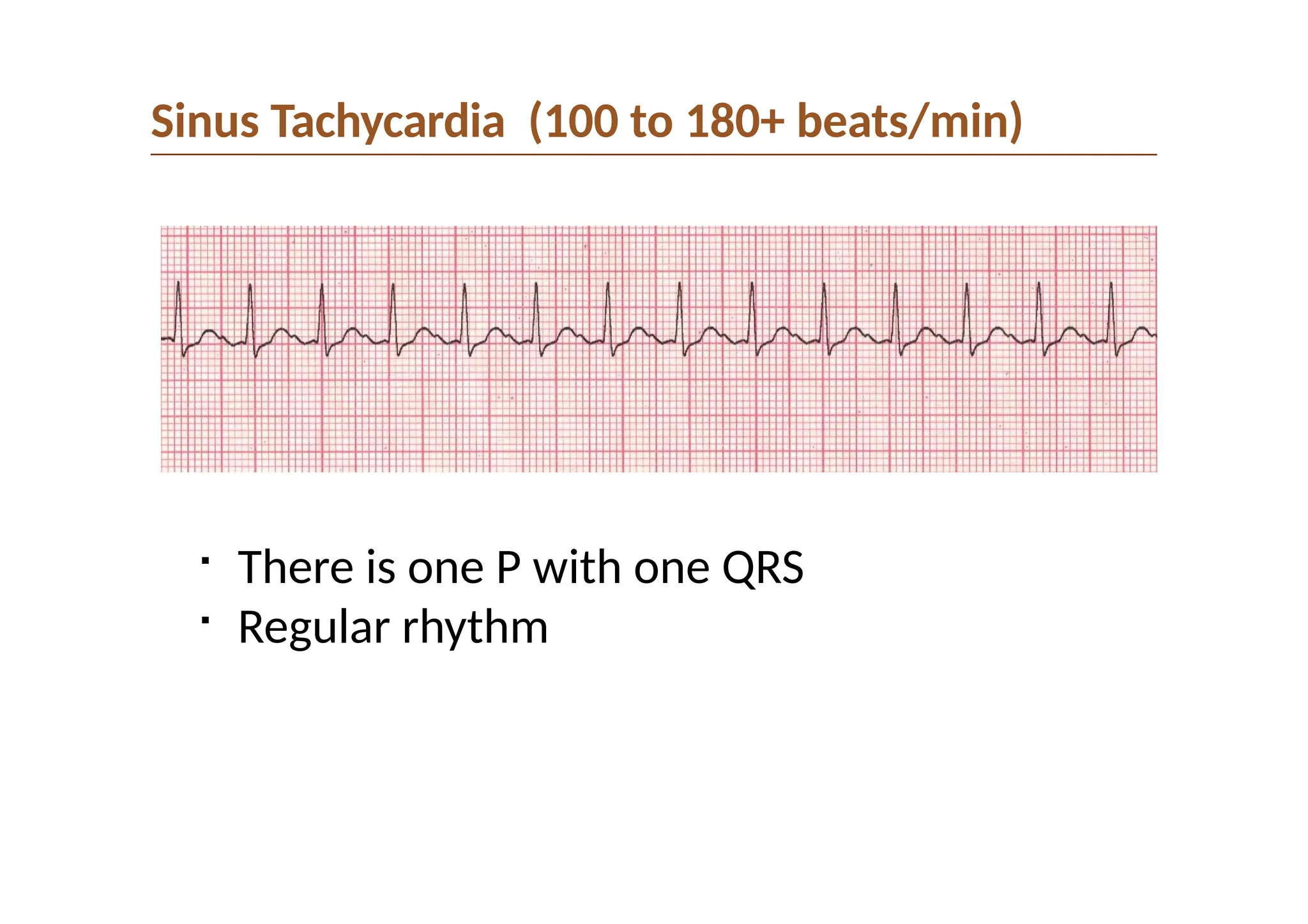
Sinus Tachycardia:
• Seekand treat underlying cause
• Do NOT treat tachycardia itself
Sinus?
(p wave before every QRS
in II or v1
Wide QRS?
(QRS ≥ 120 ms)
Ventricular Tachycardia:
• Give amiodorone or lidocaine
• and/or synchronized cardioversion
• If irregular, consider torsades give
magnesium
Unstable?
(Hypotension, altered
mental status)
Unstable Non-Sinus Tachycardia:
• Perform SYNCHRONIZED
cardioversion
Irregular?
Atrial Fibrillation with Rapid Ventricular Response
• Rate control: Consider fluids (if hypovolemic),
beta blocker if BP OK (IV best), amiodorone or
digoxin
• Anticoagulation with heparin or LMWH unless
contraindication
• Suspect and rule out structural heart disease,
especially mitral stenosis
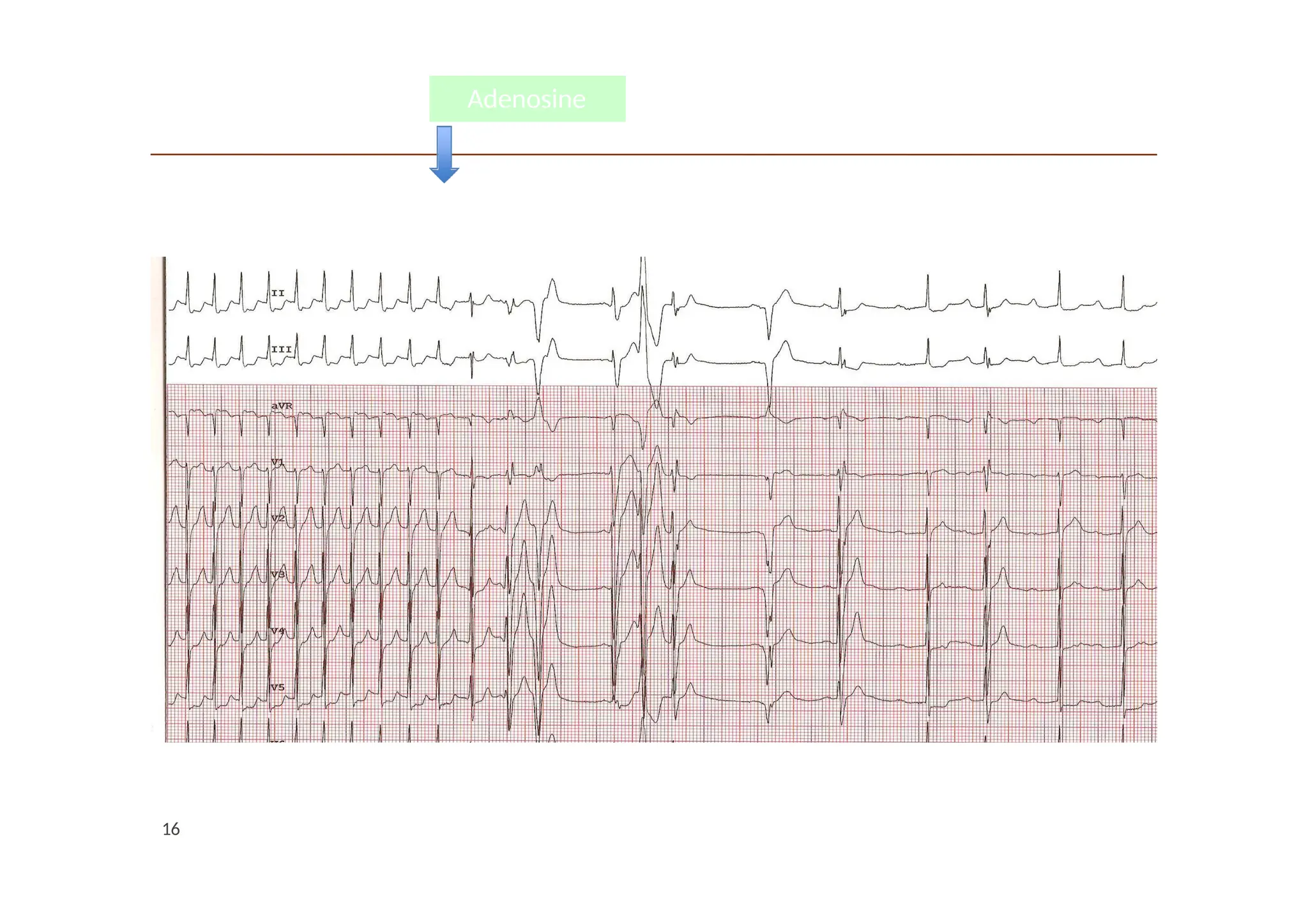
Supraventricular Tachycardia
• Vagal maneuvers
• Adenosine
YES
YES
YES
YES
NO
NO
NO
NO
11.
Narrow Complex Tachycardia
Whatare the questions to ask?
Is the rhythm regular or irregular?
Is there P with everything QRS or is P > QRS?
Regular : ST;SVT
Irregular : A fib
Sinus Tachycardia
Causes
• Hypovolemia(blood loss, dehydration)
• Fever
• Respiratory distress
• Heart failure
• Hyperthyroidism
• Certain drugs (e.g., bronchodilators)
• Physiologic states (exercise, excitement, etc.)
Treatment
• Seek and treat underlying cause
• Do NOT treat tachycardia itself
14.
SVT
• Atrial ratebetween 140 and 280 bpm
• Regular with narrow QRS unless aberrancy
• USUALLY DO NOT SEE P WAVES
• May be paroxysmal or be brought on by caffeine, exertion,
alcohol, salbutamol, or amphetamines
• Women > Men
• Young and healthy or people with structural heart disease
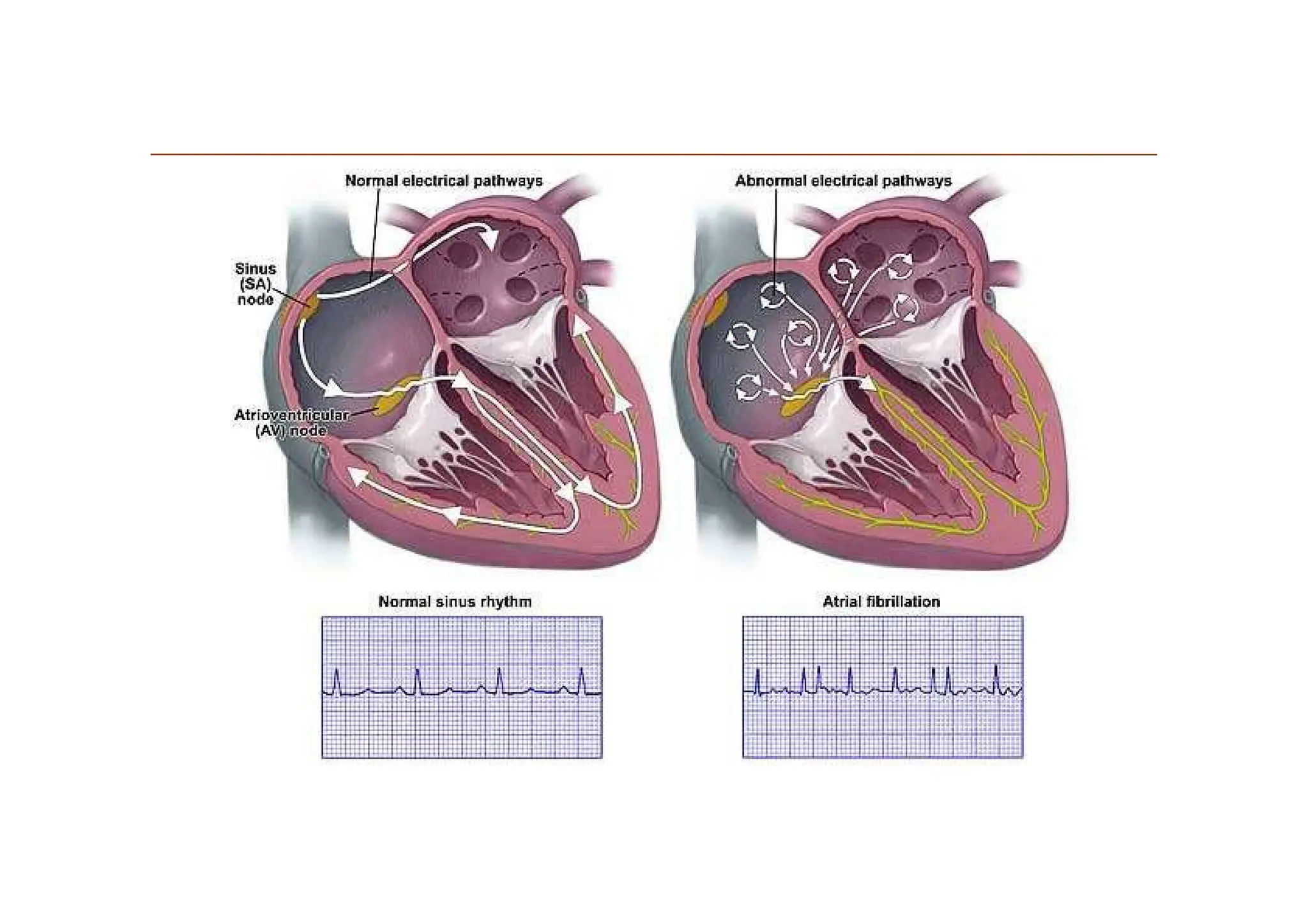
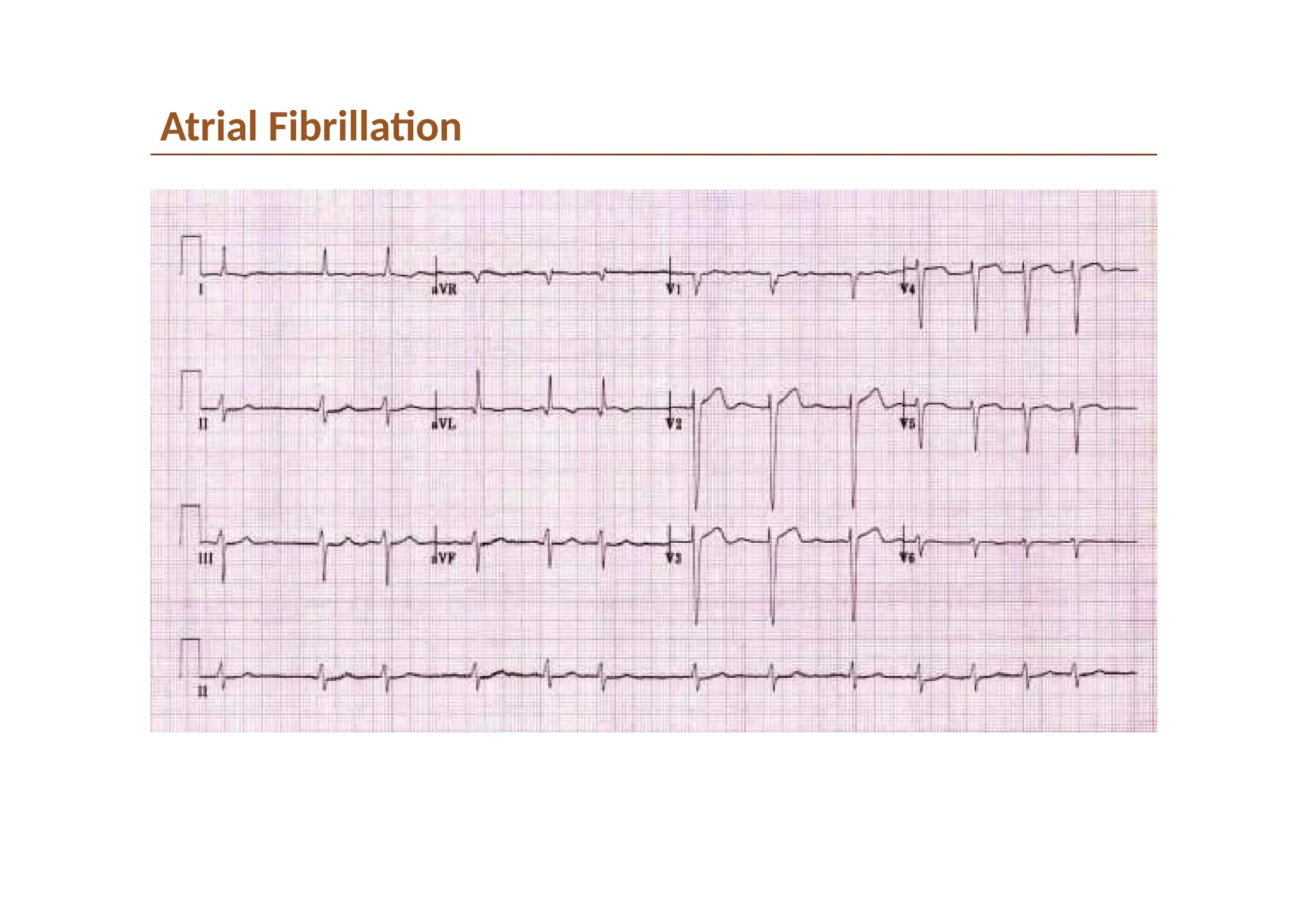
Atrial Fibrillation
• Irregularlyirregular
• NO P WAVES
• Absence of isoelectric baseline
• Variable ventricular rate (therefore irregular)
• QRS narrow unless BBB, acc path or aberrancy
• May have fibrillatory waves that mimic P waves, they are
either fine or course (amplitude)
Atrial Fibrillation
Management
• Firstdiagnose it! Do an EKG.
• Stable or Unstable?
• Rate or rhythm control?
• Assessment of Duration
Less than 48 hours or greater than 48 hours as this
determines who is safe for cardioversion
• Assessment for anticoagulation- CHADS 2 Score
• Treatment of underlying disease
22.
Atrial Fibrillation
Unstable
• Shock(120-200J)
– Might not work!
• A heart that has been
in afib can get used to
it
• Consider IVF
– Dehydration is a
common cause driving
rapid heart rates in afib
– May be in heart failure
so carefully!
• Load with amiodorone,
digoxin
Stable
Rate Control
• Atenolol (not in acute heart
failure)
• Calcium Channel Blocker
• Digoxin oral
load- better if
LVD Arrythmias,
Rhythm control
• Amiodarone Load
150mg IV
23.
Wide ComplexTachycardias
23
What arethe questions to ask?
Is the rhythm regular or irregular?
Regular :VT (monomorphic and polymorphic)
Irregular :VF
24.
Ventricular tachycardia
•
Wide complextachycardia
•
May be monomorphic or polymorphic
• Originates from single focus within the ventricles
• Produces uniform QRS complexes
25.
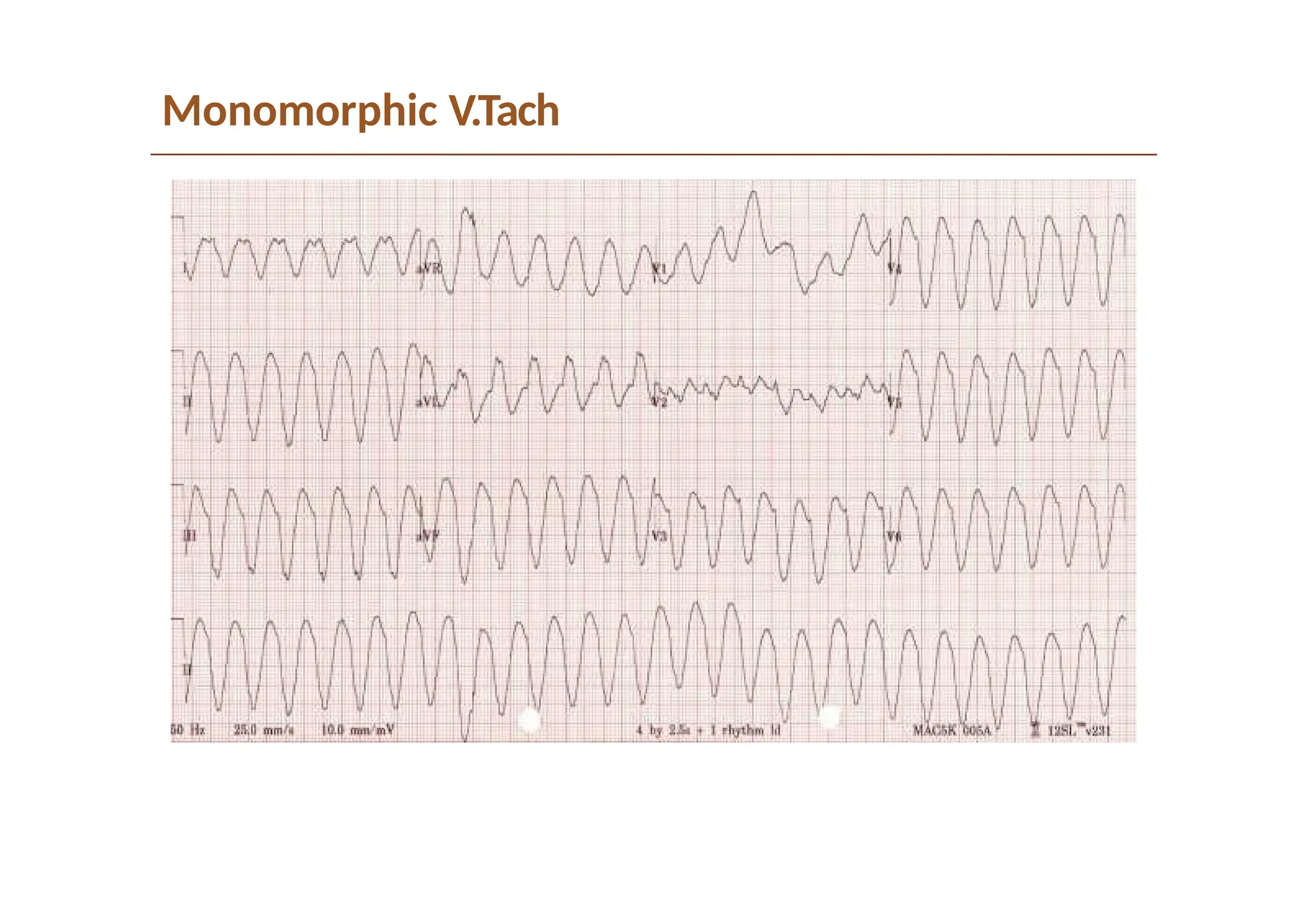
Monomorphic Ventricular Tachycardia
CAUSES
•Dilated Cardiomyopathy
• Hypertrophic Cardiomyopathy
• Ischemic Heart disease
• Chaga’s Disease
TREATMENT
• STABLE = Give drugs or DC Cardioversion
• Presence or absence of Left Ventricular Dysfunction determines
choice of pharmacologic therapy
– Amiodarone 150 mg I.V. over 10 minutes may be RX of choice
maximum 2.2 gm/24 hours
• UNSTABLE? (hypotension, chest pain, cardiac failure, ALOC)
• = DC Cardioversion (Biphasic 100-200 J with sedation)
Polymorphic VT/Torsade dePointes
•
Classic pattern of “twisting” of QRS in an axis
•
Can be seen with electrolyte abnormalities- Hypo K,
Hypo Mg
28.
Polymorphic VT
• Requiresimmediate defibrillation as does VF
• Drug of choice I.V. Lidocaine , Amiodarone
• Usually result of severe metabolic disturbance or Cardiac
ischemia.
• Rarely when associated with prolonged QT known as Torsades
de Pointes
• Magnesium replacement therapy/replete potassium (even if
normal)
28
29.
“Torsade de Pointes”(PolymorphicVT Associated with
Prolonged Repolarization)
• Occurs in the context of QT prolongation
• QRS “twists” around isoelectric line
• Must have PVT + QT prolongation
• Can be short lived and self terminating but CAN progress into
ventricular fibrillation
• Bigeminy in someone with prolonged QT may give a warning
they will go into Torsades
29
30.
Torsades de Points
•QTC is prolonged if > 440ms in men or >460ms in women
• QTC >500 is associated with increased risk of Torsades
Must Ask Why QT prolongation? Will help treatment
• Drugs effects?
• Electrolyte Abnormalities: Hypokalemia,
Hypomagnesaemia, Hypocalcemia
• Hypothermia
• Raised increased intracranial pressure
• Congenital
• Myocardial Ischemia
• TREATMENT: CARDIOVERSION + MAGNESIUM 2-4G IV
31.
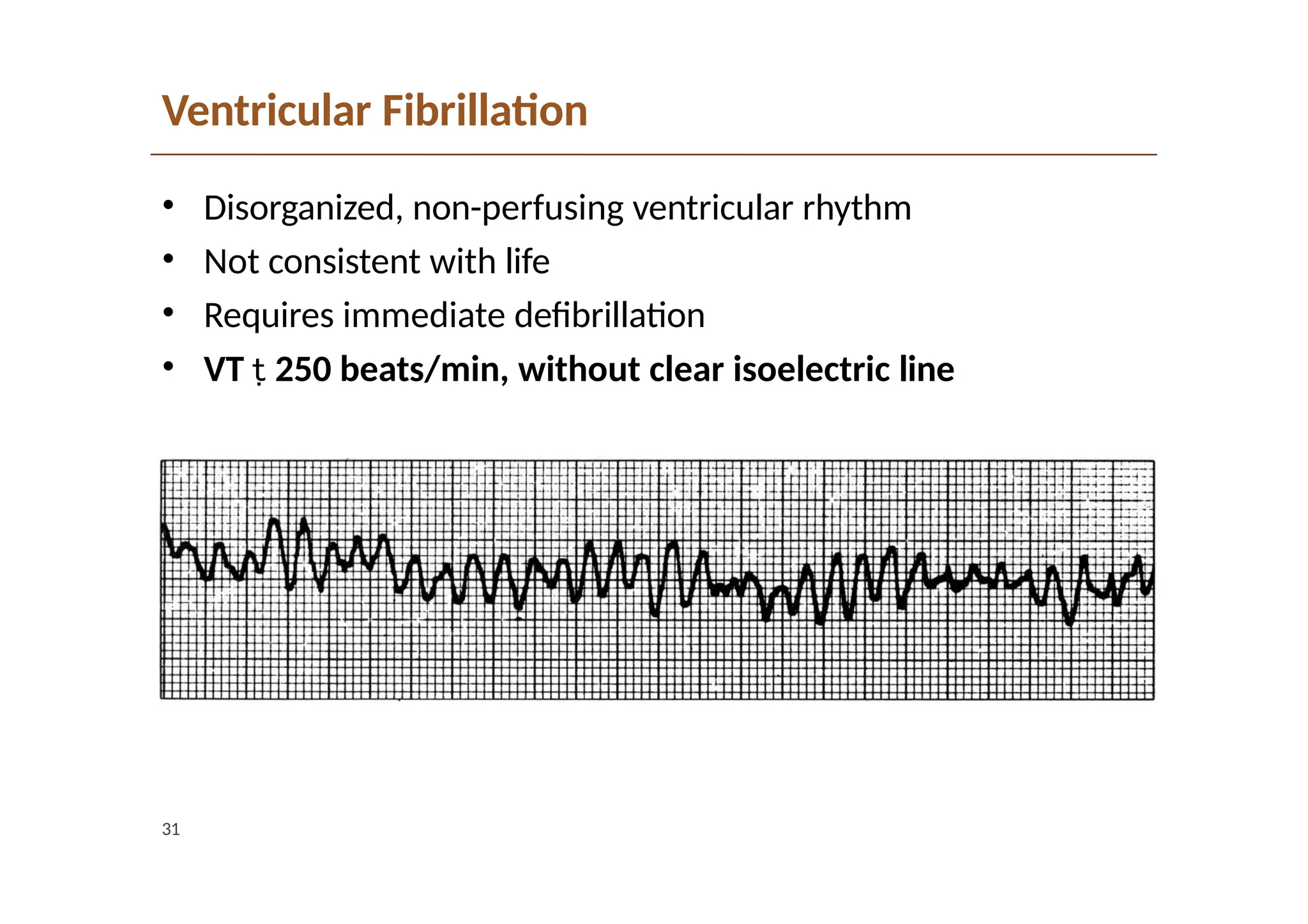
Ventricular Fibrillation
• Disorganized,non-perfusing ventricular rhythm
• Not consistent with life
• Requires immediate defibrillation
• VT 250 beats/min, without clear isoelectric line
31
32.
Ventricular Fibrillation
32
• CardiopulmonaryResuscitation (CPR): High quality
compressions!!! Limit interruptions in CPR
• Success decrease 10% per minute in VF
• Defibrillate: adults: biphasic: 200 J once – 5 cycles
of CPR
• Administer epinephrine 1 mg every 3–5 minutes
• Administer amiodarone 300 mg IV/IO once, then consider
administering an additional 150 mg once
• Consider lidocaine if no response
33.
Case 2
• 24yo EKG tech p/w heart palpitations, shortness of breath.
Appears anxious.
• What is the DDx/approach to narrow complex tachycardia?
81






























![Cardiccccac Arrhythmias [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cardiacarrhythmiasautosaved-241108153215-72acce97-thumbnail.jpg?width=640&height=640&fit=bounds)





































