The document provides an overview of electrocardiography (ECG) including:
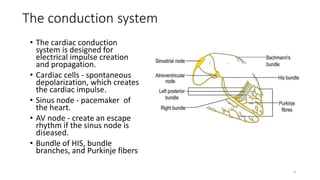
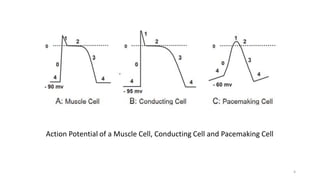
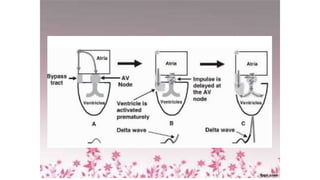
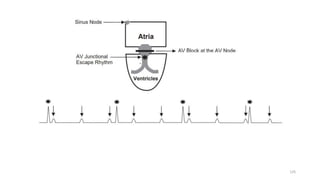
1) It describes the cardiac conduction system and the three types of heart cells.
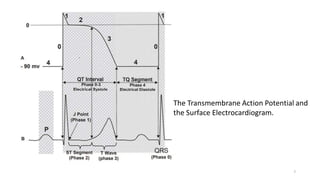
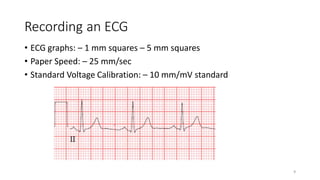
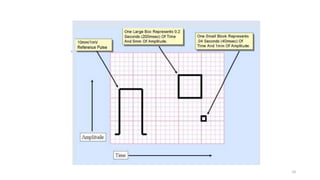
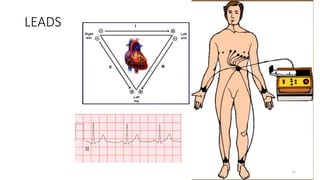
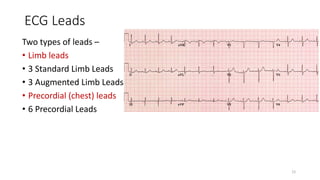
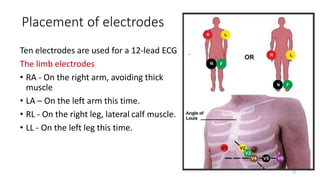
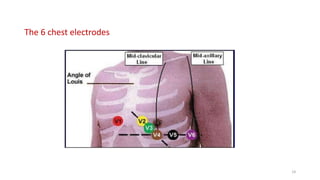
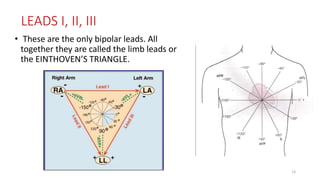
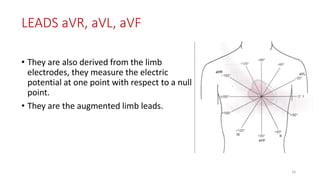
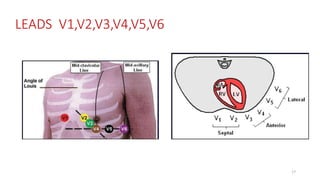
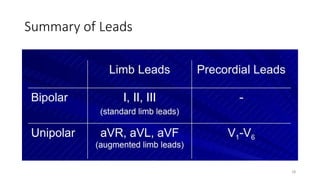
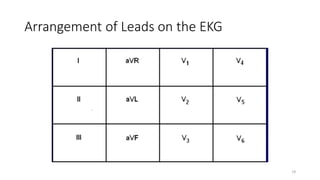
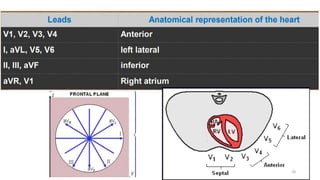
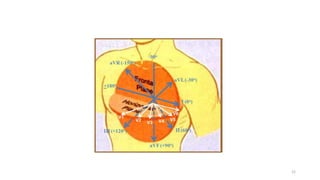
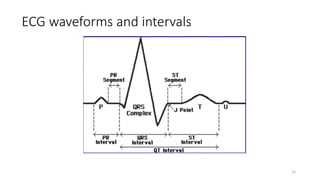
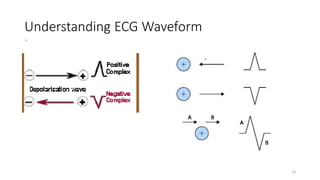
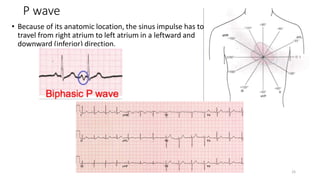
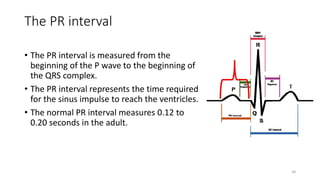
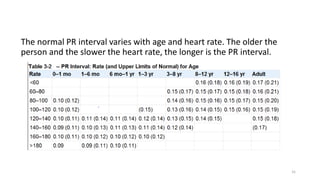
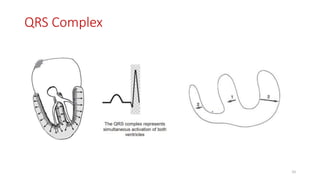
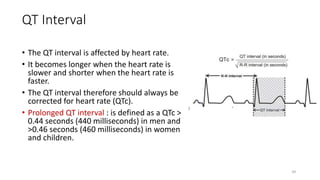
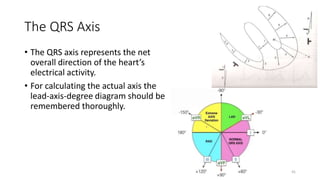
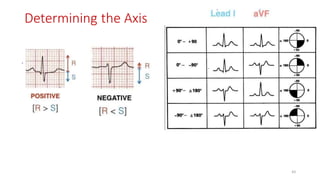
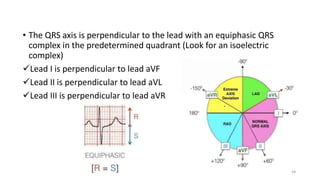
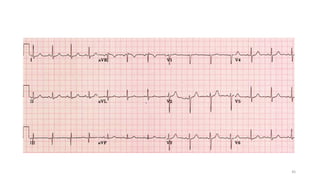
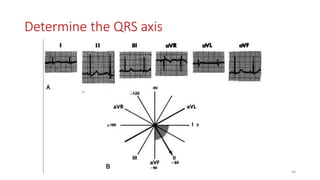
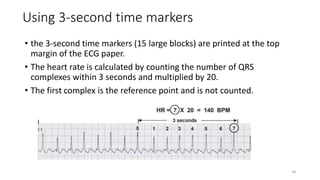
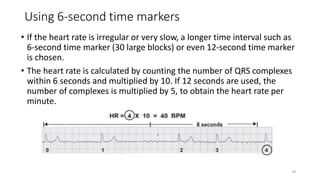
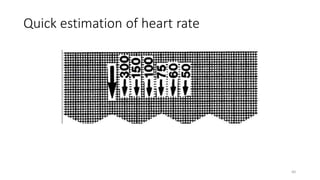
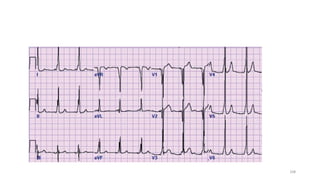
2) It explains the basics of an ECG including the leads, waveforms, intervals and how to determine heart rate.
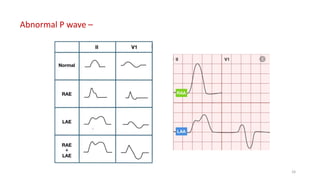
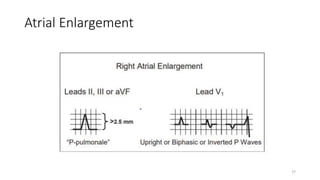
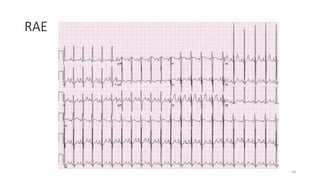
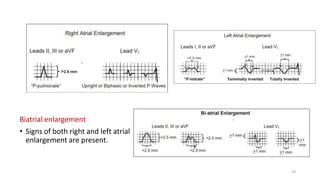
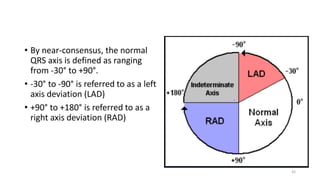
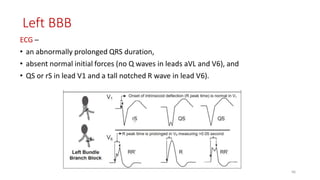
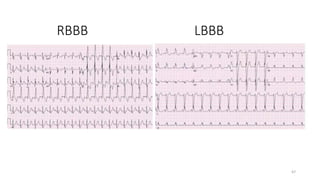
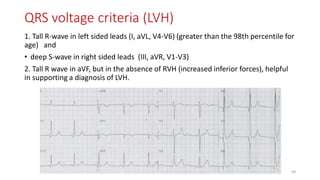
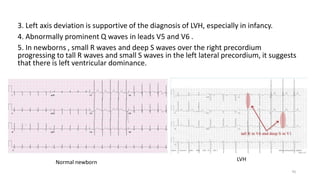
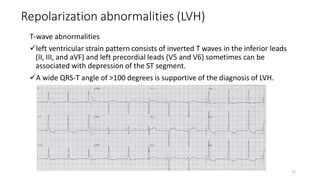
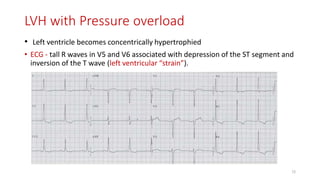
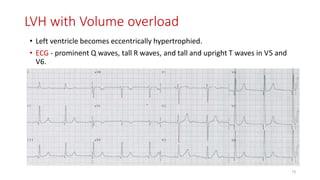
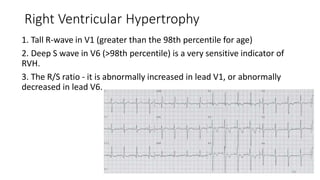
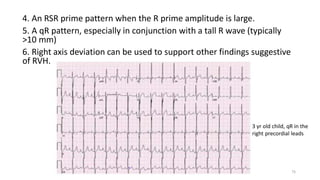
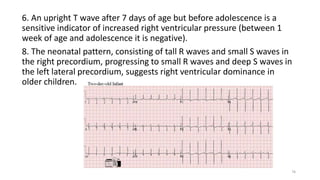
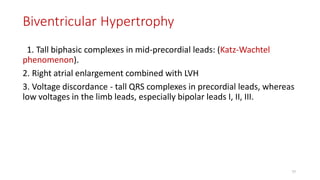
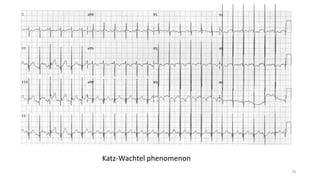
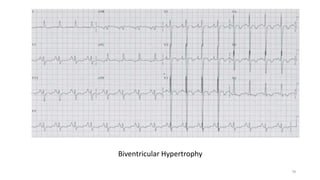
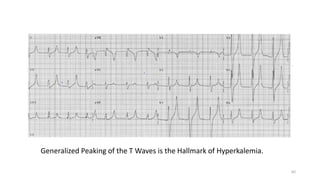
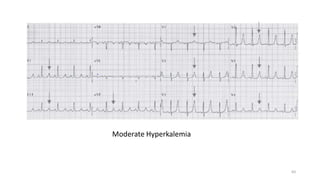
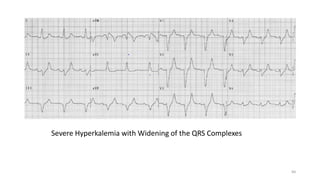
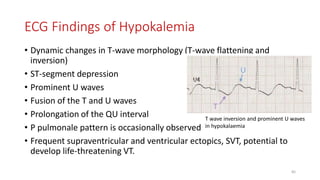
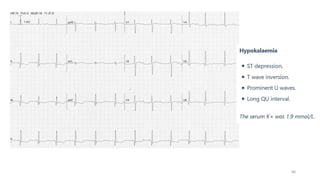
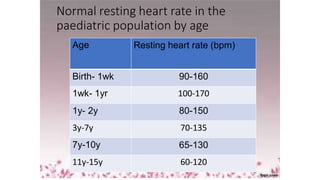
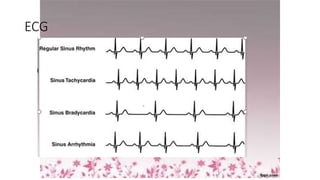
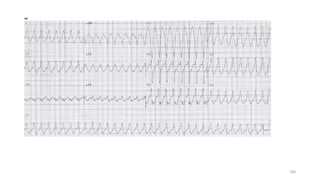
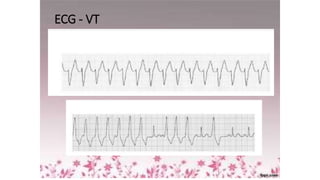
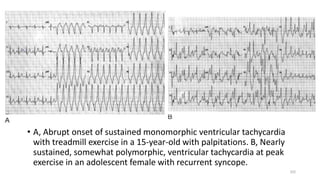
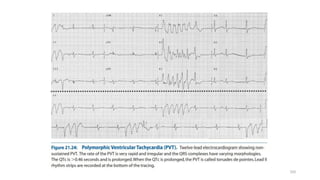
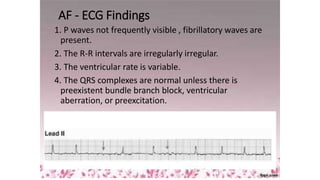
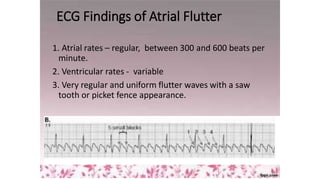
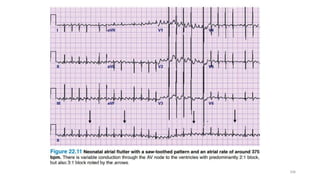
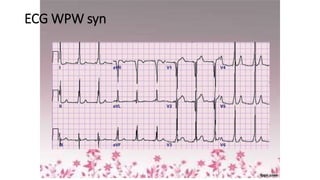
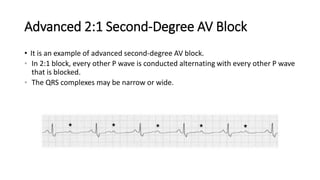
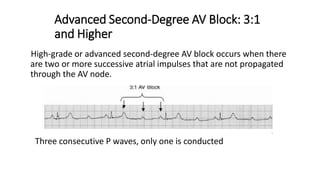
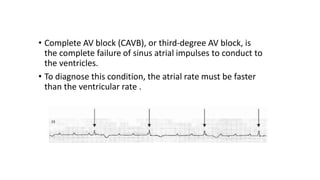
3) It discusses abnormalities that can be seen on ECG such as bundle branch blocks, chamber enlargement, and arrhythmias.