Downloaded 347 times

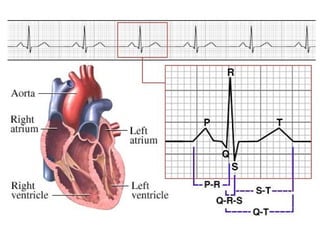
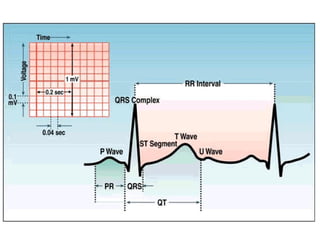
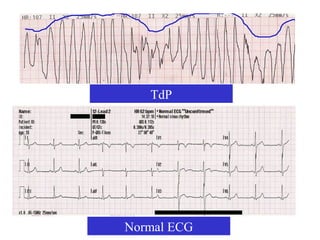
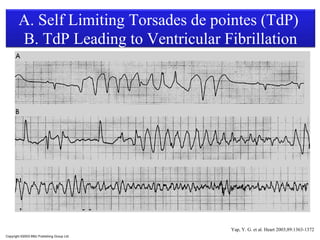
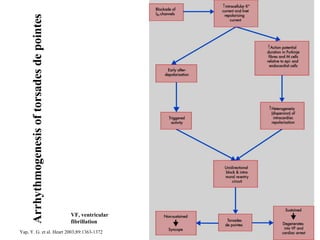
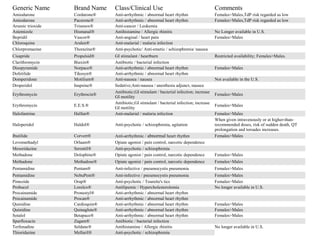
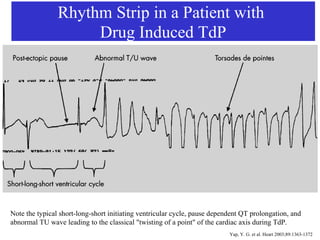
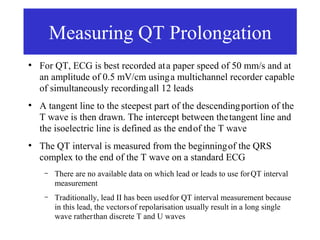
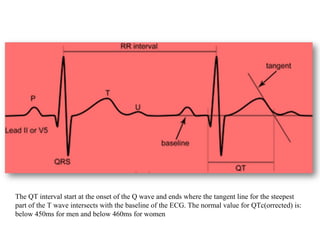
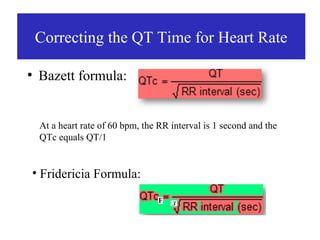
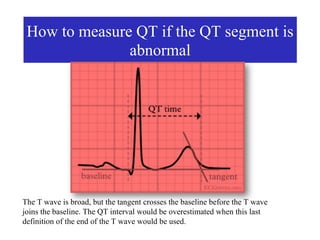
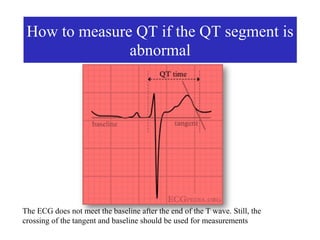
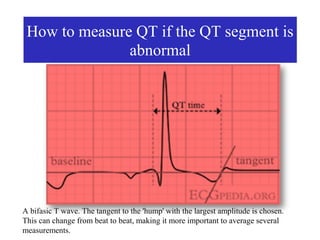
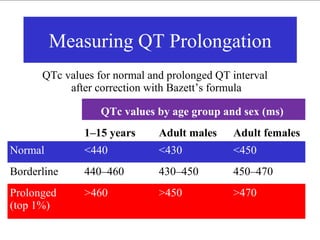
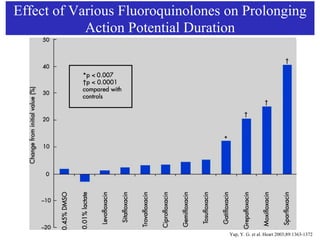
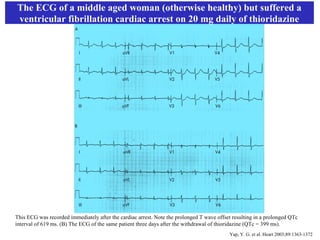
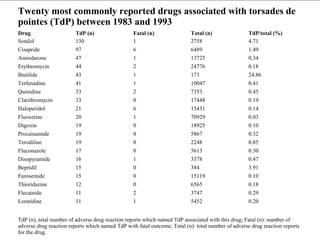


This document discusses QT prolongation and Torsades de Pointes (TdP), a type of ventricular arrhythmia. It provides background on the QT interval and factors that can cause prolongation and TdP. Certain drugs are noted to block potassium channels and prolong the QT interval, with some drugs like cisapride, erythromycin, and sotalol commonly associated with TdP. The document outlines how to measure the QT interval and correct it for heart rate, and notes values that indicate normal vs prolonged intervals. Images of ECG strips demonstrate characteristic patterns seen with TdP.











































































































