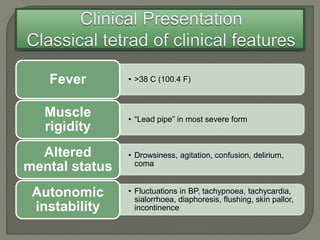
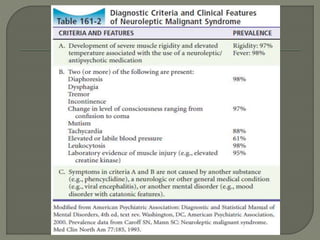
This document describes the case of a 53-year-old lady brought in with altered mental status and fever. Her symptoms worsened after 12 hours, with increased confusion and rigidity. This was likely caused by neuroleptic malignant syndrome (NMS), a rare but serious reaction to antipsychotic drugs. NMS requires immediate withdrawal of antipsychotics, supportive care, and may include benzodiazepines or dopaminergic drugs. Careful monitoring is needed if antipsychotics are reintroduced.























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






