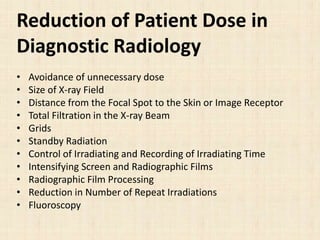
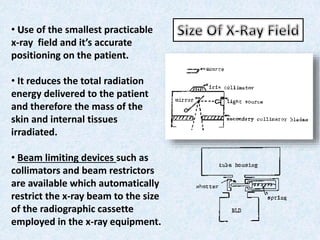
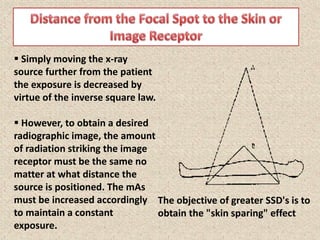
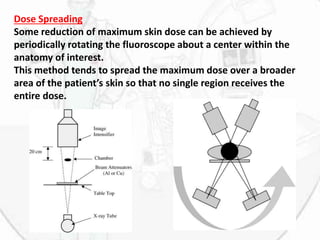


This document summarizes techniques to reduce radiation dose in diagnostic radiology, including fluoroscopy. It discusses using the smallest x-ray field, increasing distance between the patient and x-ray source, using filters, grids, and intensifying screens. It also covers automatic processing, avoiding unnecessary repeat images, and techniques to reduce dose in fluoroscopy like intermittent exposure, removal of grids, and last image hold. The document emphasizes training operators and using radiation only when necessary to obtain diagnostic information.









































































