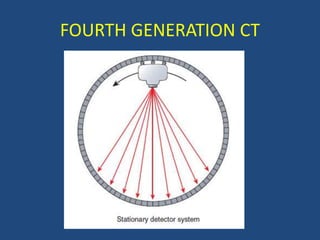
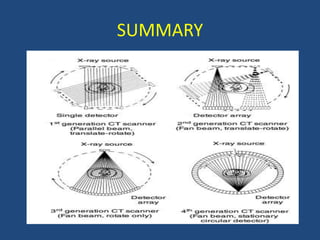
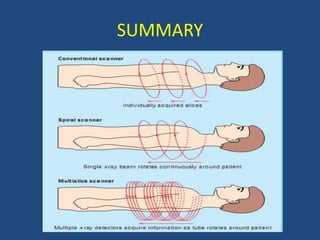
This document discusses the history and evolution of different generations of computed tomography (CT) technology. It describes the key limitations and innovations of each generation from the first generation CT scanner created in 1971, which took 5 minutes to produce an image, to modern multi-slice CT scanners. The higher the generation number, the faster imaging times and more slices that could be acquired simultaneously. However, a higher generation does not always indicate a higher performance system.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


