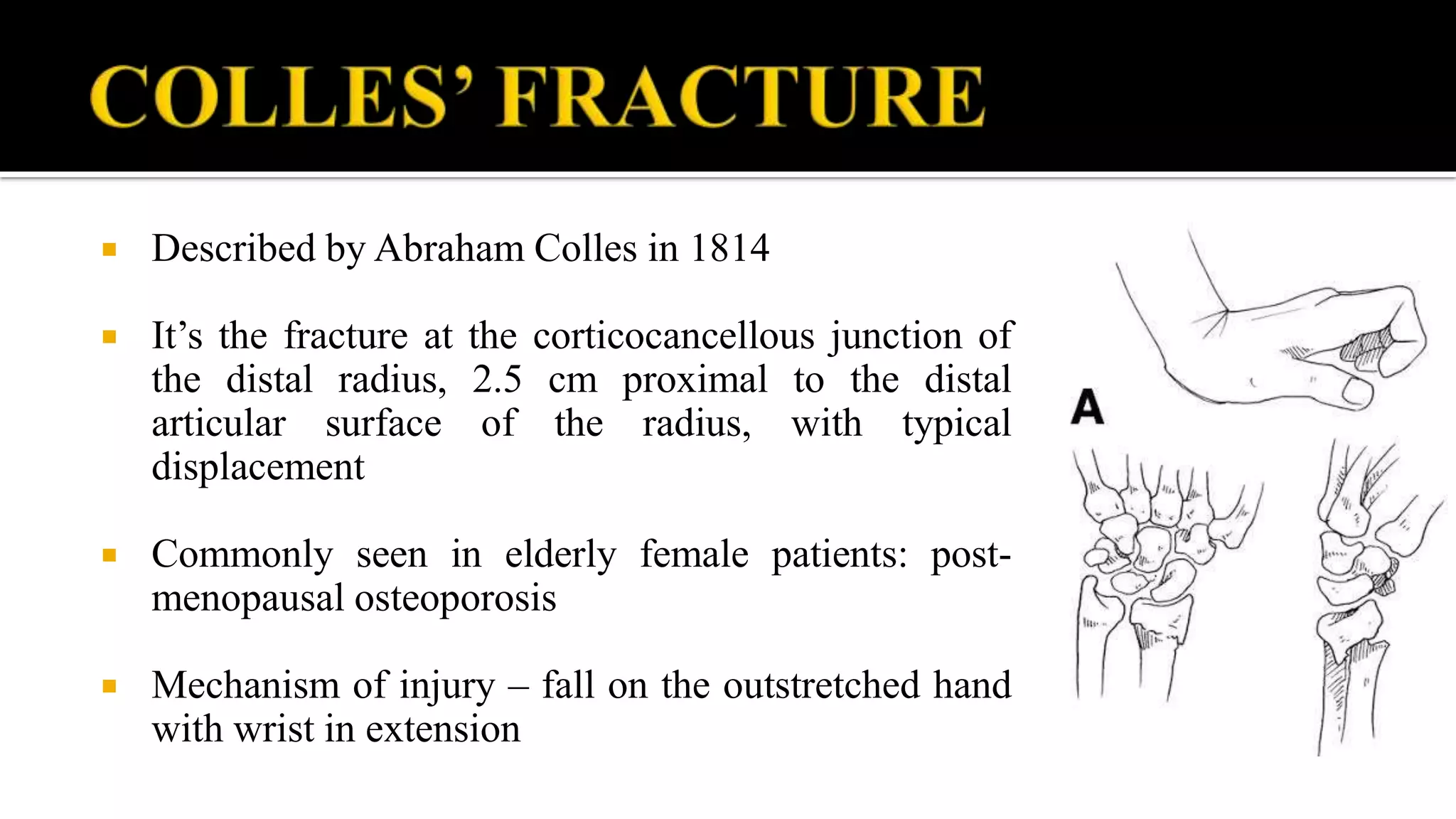
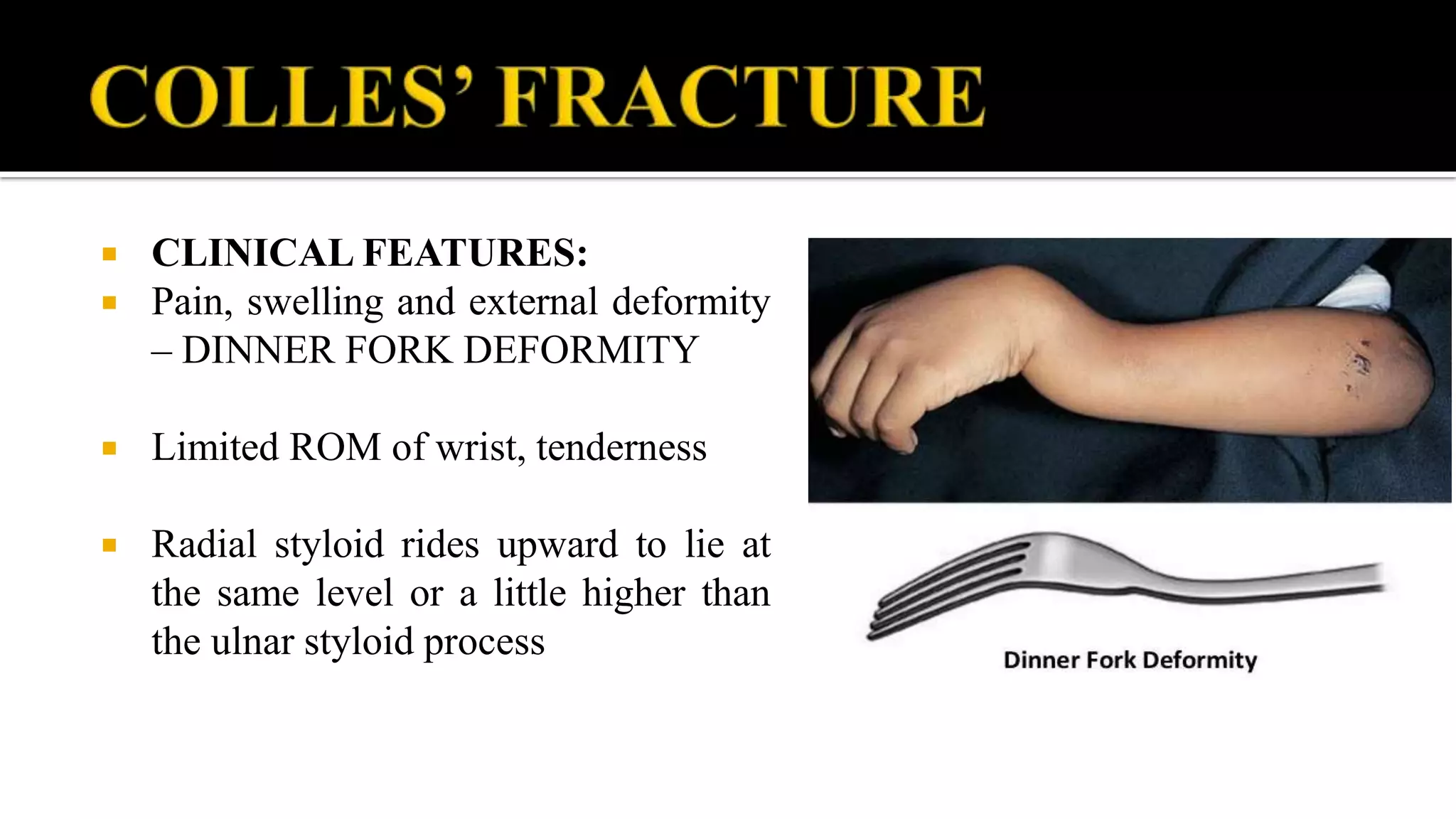
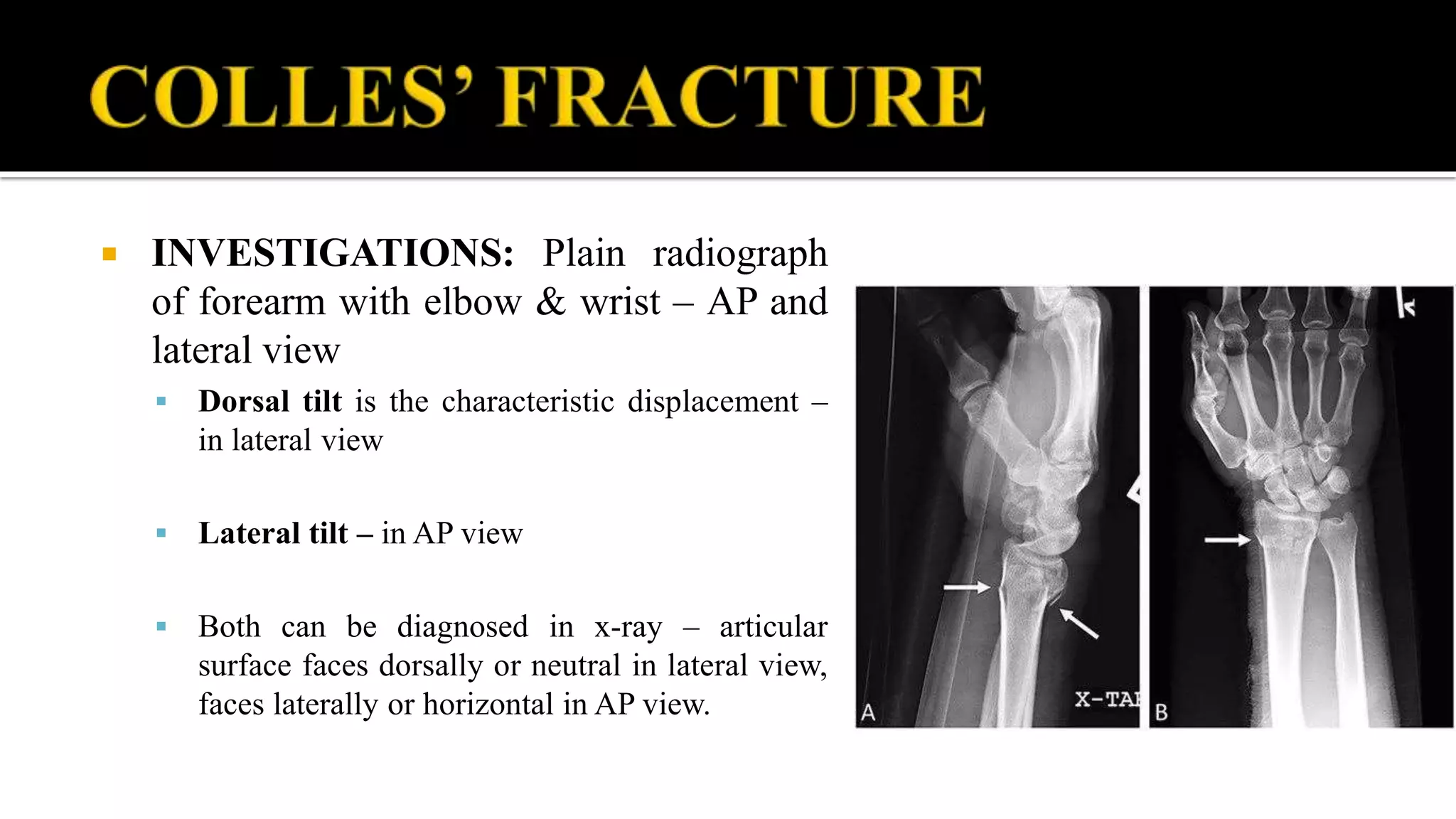
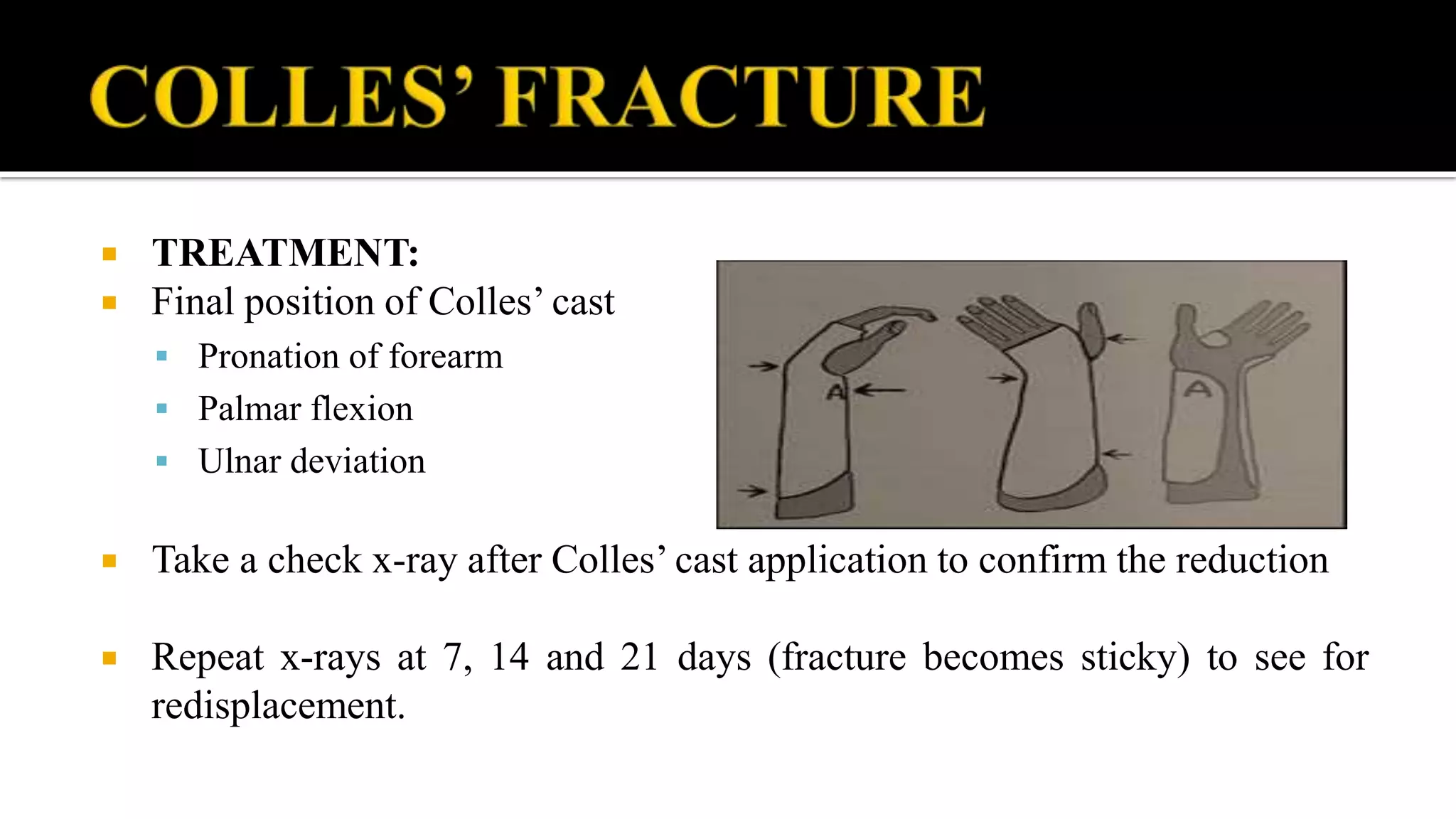
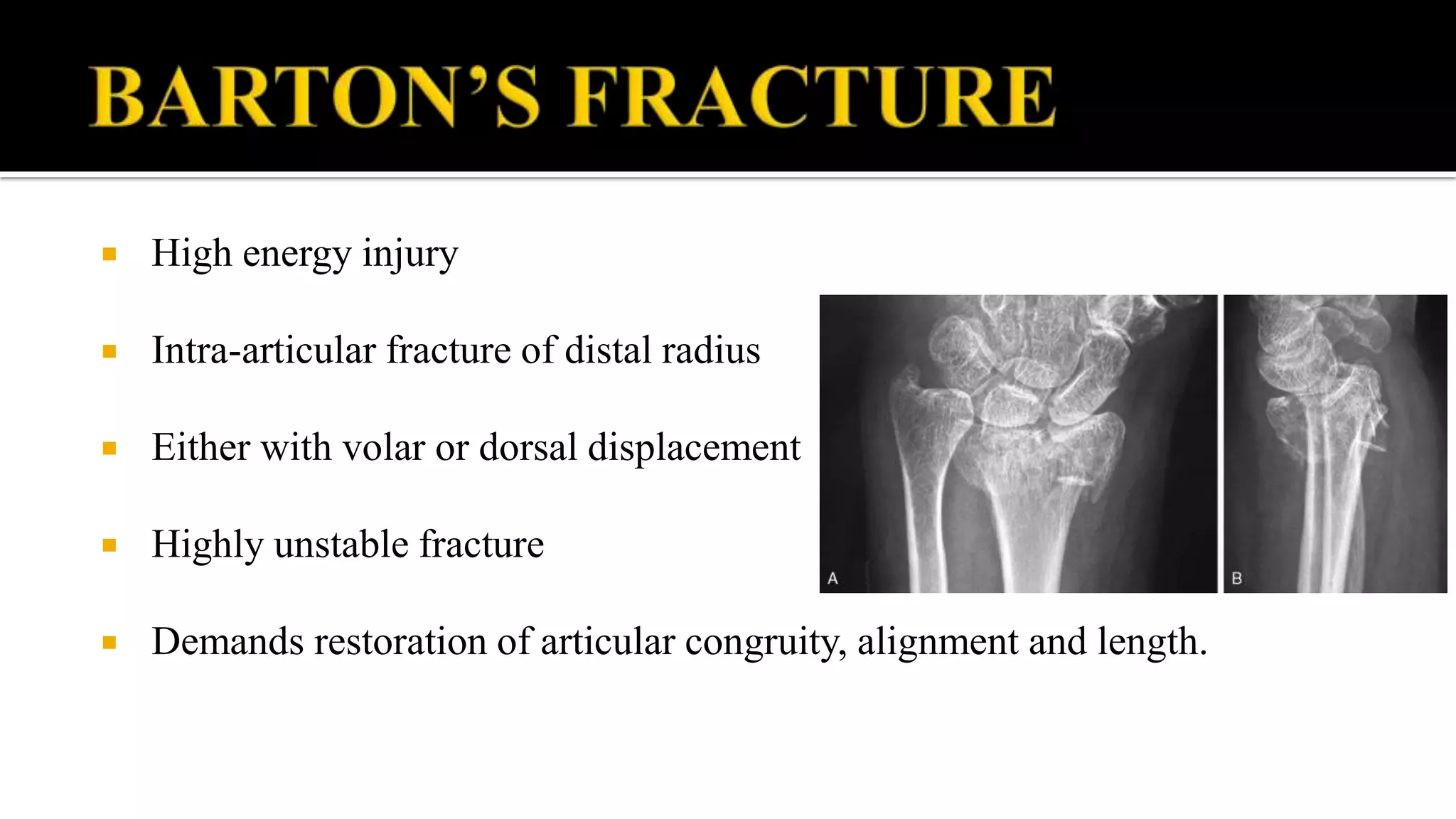
This document discusses Colles' fracture, which is a fracture of the distal radius near the wrist. It most commonly occurs in post-menopausal women after a fall on an outstretched hand. The fracture causes dorsal displacement of the distal radius fragment. Treatment involves closed manipulation and casting the forearm in pronation, palmar flexion, and ulnar deviation. Complications can include nerve injuries, complex regional pain syndrome, malunion from improper treatment, and secondary osteoarthritis in more severe fractures.