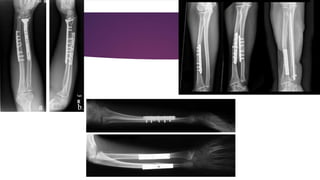
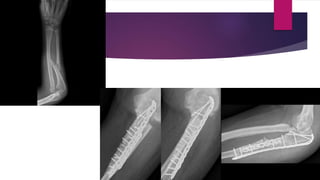
This document discusses fractures of the forearm and wrist. It describes the Colles' fracture, which occurs at the distal end of the radius when falling onto an outstretched hand. It can be stable or unstable based on comminution. Treatment involves closed or open reduction and cast immobilization. Smith's fractures of the distal radius require supination to reduce. Shaft fractures of the radius and ulna usually require open reduction due to instability. Galeazzi and Monteggia fracture-dislocations involve both a bone fracture and joint dislocation, requiring open reduction and internal fixation for treatment. Complications include malunion and loss of function.





![FOREARM_FRACTURES[1].pptx and management](https://cdn.slidesharecdn.com/ss_thumbnails/forearmfractures1-250813120934-75e3f6d7-thumbnail.jpg?width=640&height=640&fit=bounds)












































