Causes of dislocation
•MCC : Traumatic
• Great and sudden force applied, by either blow or fall, to the joint causes the
bones in the joint to displaced.
5.
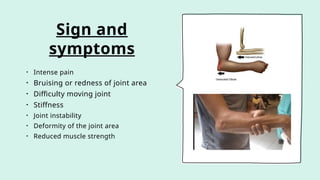
Sign and
symptoms
• Intensepain
• Bruising or redness of joint area
• Difficulty moving joint
• Stiffness
• Joint instability
• Deformity of the joint area
• Reduced muscle strength
6.
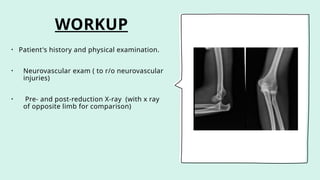
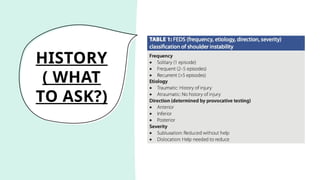
WORKUP
• Patient's historyand physical examination.
• Neurovascular exam ( to r/o neurovascular
injuries)
• Pre- and post-reduction X-ray (with x ray
of opposite limb for comparison)
7.
Principle of treatment
•Reduce the dislocated joint as soon as possible under sedation /general
anaesthesia
• Check neurovascular function distally
• Take post reduction radiograph
• Immobilize the joint
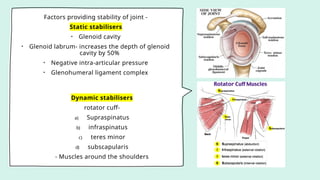
Factors providing stabilityof joint -
Static stabilisers
• Glenoid cavity
• Glenoid labrum- increases the depth of glenoid
cavity by 50%
• Negative intra-articular pressure
• Glenohumeral ligament complex
Dynamic stabilisers
rotator cuff-
a) Supraspinatus
b) infraspinatus
c) teres minor
d) subscapularis
- Muscles around the shoulders
11.
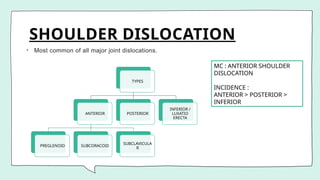
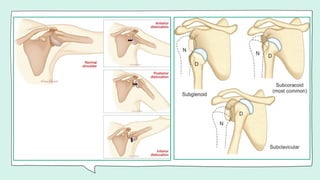
SHOULDER DISLOCATION
• Mostcommon of all major joint dislocations.
TYPES
ANTERIOR
PREGLENOID SUBCORACOID
SUBCLAVICULA
R
POSTERIOR
INFERIOR /
LUXATIO
ERECTA
MC : ANTERIOR SHOULDER
DISLOCATION
INCIDENCE :
ANTERIOR > POSTERIOR >
INFERIOR
13.
ANTERIOR
DISLOCATION
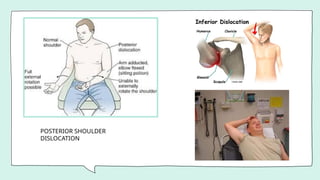
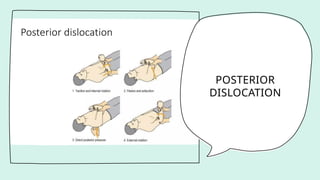
POSTERIOR
DISLOCATION
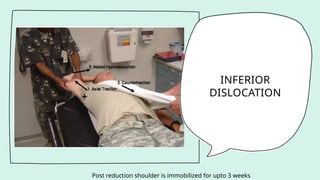
INFERIOR
DISLOCATION
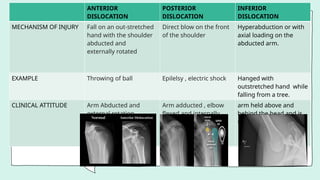
MECHANISM OF INJURYFall on an out-stretched
hand with the shoulder
abducted and
externally rotated
Direct blow on the front
of the shoulder
Hyperabduction or with
axial loading on the
abducted arm.
EXAMPLE Throwing of ball Epilelsy , electric shock Hanged with
outstretched hand while
falling from a tree.
CLINICAL ATTITUDE Arm Abducted and
external rotation
Arm adducted , elbow
flexed and internally
rotated
arm held above and
behind the head and is
unable to adduct arm
14.
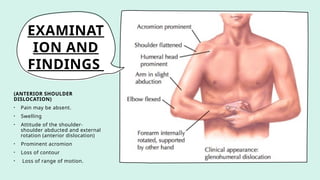
EXAMINAT
ION AND
FINDINGS
(ANTERIOR SHOULDER
DISLOCATION)
•Pain may be absent.
• Swelling
• Attitude of the shoulder-
shoulder abducted and external
rotation (anterior dislocation)
• Prominent acromion
• Loss of contour
• Loss of range of motion.
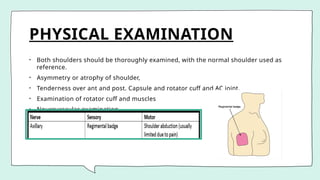
PHYSICAL EXAMINATION
• Bothshoulders should be thoroughly examined, with the normal shoulder used as
reference.
• Asymmetry or atrophy of shoulder,
• Tenderness over ant and post. Capsule and rotator cuff and AC joint.
• Examination of rotator cuff and muscles
• Neurovascular examination.
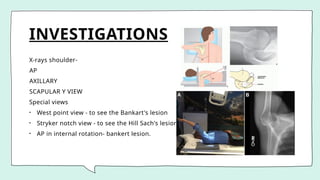
INVESTIGATIONS
X-rays shoulder-
AP
AXILLARY
SCAPULAR YVIEW
Special views
• West point view - to see the Bankart's lesion
• Stryker notch view - to see the Hill Sach's lesion
• AP in internal rotation- bankert lesion.
20.
• CT withthree dimensional view most sensitive test for detecting and measuring
bone deficiency or retroversion of the glenoid or humerus.
• MRI- imp. For shoft tissue pathology.
• Arthrgraphy-xray or CT arthrography can show capsular laxity, tear, soft tissue
abnormality and bony abnormality.
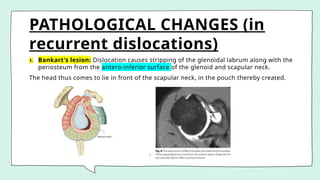
PATHOLOGICAL CHANGES (in
recurrentdislocations)
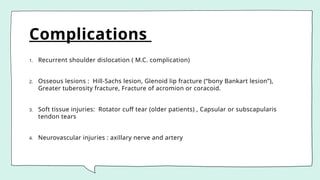
1. Bankart's lesion: Dislocation causes stripping of the glenoidal labrum along with the
periosteum from the antero-inferior surface of the glenoid and scapular neck.
The head thus comes to lie in front of the scapular neck, in the pouch thereby created.
23.
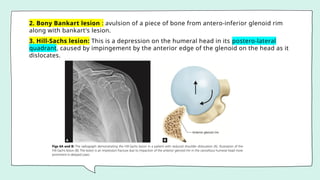
2. Bony Bankartlesion : avulsion of a piece of bone from antero-inferior glenoid rim
along with bankart's lesion.
3. Hill-Sachs lesion: This is a depression on the humeral head in its postero-lateral
quadrant, caused by impingement by the anterior edge of the glenoid on the head as it
dislocates.
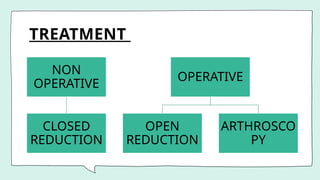
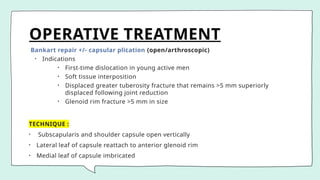
OPERATIVE TREATMENT
Bankart repair+/- capsular plication (open/arthroscopic)
• Indications
• First-time dislocation in young active men
• Soft tissue interposition
• Displaced greater tuberosity fracture that remains >5 mm superiorly
displaced following joint reduction
• Glenoid rim fracture >5 mm in size
TECHNIQUE :
• Subscapularis and shoulder capsule open vertically
• Lateral leaf of capsule reattach to anterior glenoid rim
• Medial leaf of capsule imbricated
30.
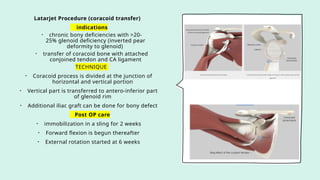
Latarjet Procedure (coracoidtransfer)
indications
• chronic bony deficiencies with >20-
25% glenoid deficiency (inverted pear
deformity to glenoid)
• transfer of coracoid bone with attached
conjoined tendon and CA ligament
TECHNIQUE
• Coracoid process is divided at the junction of
horizontal and vertical portion
• Vertical part is transferred to antero-inferior part
of glenoid rim
• Additional iliac graft can be done for bony defect
Post OP care
• immobilization in a sling for 2 weeks
• Forward flexion is begun thereafter
• External rotation started at 6 weeks
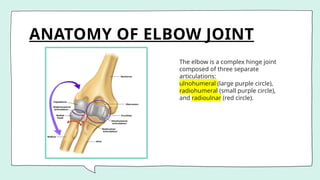
ANATOMY OF ELBOWJOINT
The elbow is a complex hinge joint
composed of three separate
articulations:
ulnohumeral (large purple circle),
radiohumeral (small purple circle),
and radioulnar (red circle).
35.
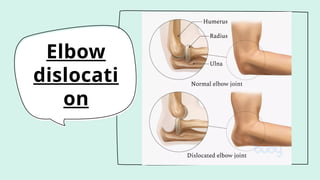
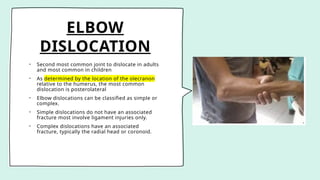
ELBOW
DISLOCATION
• Second mostcommon joint to dislocate in adults
and most common in children
• As determined by the location of the olecranon
relative to the humerus, the most common
dislocation is posterolateral
• Elbow dislocations can be classified as simple or
complex.
• Simple dislocations do not have an associated
fracture most involve ligament injuries only.
• Complex dislocations have an associated
fracture, typically the radial head or coronoid.
36.
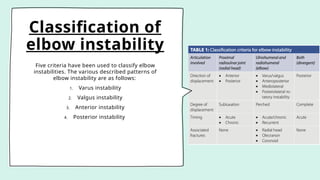
Classification of
elbow instability
Fivecriteria have been used to classify elbow
instabilities. The various described patterns of
elbow instability are as follows:
1. Varus instability
2. Valgus instability
3. Anterior instability
4. Posterior instability
37.
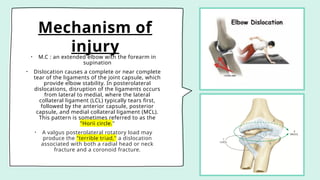
Mechanism of
injury
• M.C: an extended elbow with the forearm in
supination
• Dislocation causes a complete or near complete
tear of the ligaments of the joint capsule, which
provide elbow stability. In posterolateral
dislocations, disruption of the ligaments occurs
from lateral to medial, where the lateral
collateral ligament (LCL) typically tears first,
followed by the anterior capsule, posterior
capsule, and medial collateral ligament (MCL).
This pattern is sometimes referred to as the
"Horii circle."
• A valgus posterolateral rotatory load may
produce the "terrible triad," a dislocation
associated with both a radial head or neck
fracture and a coronoid fracture.
38.
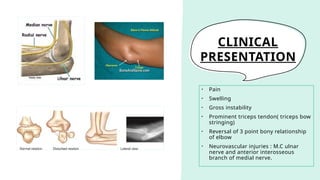
CLINICAL
PRESENTATION
• Pain
• Swelling
•Gross instability
• Prominent triceps tendon( triceps bow
stringing)
• Reversal of 3 point bony relationship
of elbow
• Neurovascular injuries : M.C ulnar
nerve and anterior interosseous
branch of medial nerve.
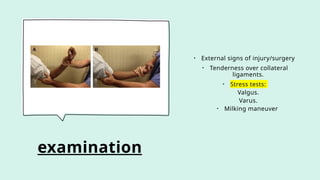
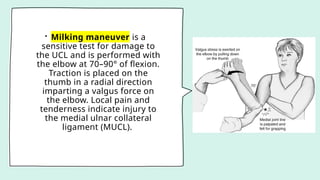
• Milking maneuveris a
sensitive test for damage to
the UCL and is performed with
the elbow at 70–90° of flexion.
Traction is placed on the
thumb in a radial direction
imparting a valgus force on
the elbow. Local pain and
tenderness indicate injury to
the medial ulnar collateral
ligament (MUCL).
41.
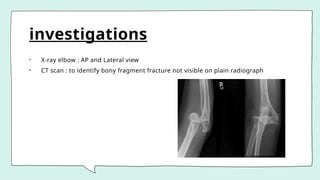
investigations
• X-ray elbow: AP and Lateral view
• CT scan : to identify bony fragment fracture not visible on plain radiograph
42.
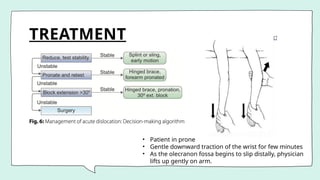
TREATMENT
• Patient inprone
• Gentle downward traction of the wrist for few minutes
• As the olecranon fossa begins to slip distally, physician
lifts up gently on arm.
43.
OPERATIVE METHODS
open reductioninternal fixation (ORIF) with ligament repair
Indications
• closed reduction cannot be performed
• often due to entrapped soft tissue or osteochondral fragments
• persistent instability after reduction
• acute complex elbow dislocations (presence of coronoid, radial head, olecranon
fractures)
Technique
ORIF of coronoid, radial head, olecranon fracture if present
ligament repair : perform LCL repair +/- MCL repair depending on intraoperative
stability
Postoperative : elbow requires >50-60° flexion to maintain reduction
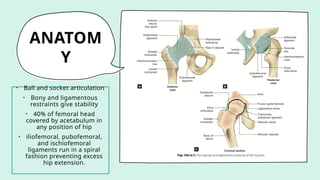
ANATOM
Y
• Ball andsocket articulation
• Bony and ligamentous
restraints give stability
• 40% of femoral head
covered by acetabulum in
any position of hip
• iliofemoral, pubofemoral,
and ischiofemoral
ligaments run in a spiral
fashion preventing excess
hip extension.
47.
MECHANISM
OF INJURY
High-energy trauma:motor vehicle accident,
fall from a height, or an industrial accident.
Force transmission to the hip joint results from
one of three common sources:
• The anterior surface of the flexed knee
striking an object
• The sole of the foot, with the ipsilateral knee
extended
• The greater trochanter
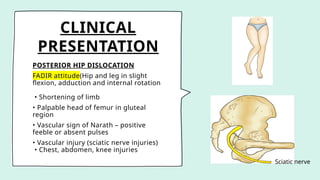
CLINICAL
PRESENTATION
POSTERIOR HIP DISLOCATION
FADIRattitude(Hip and leg in slight
flexion, adduction and internal rotation
• Shortening of limb
• Palpable head of femur in gluteal
region
• Vascular sign of Narath – positive
feeble or absent pulses
• Vascular injury (sciatic nerve injuries)
• Chest, abdomen, knee injuries
Sciatic nerve
50.
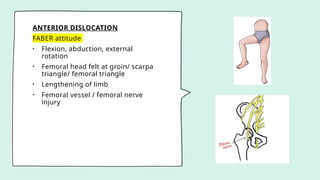
ANTERIOR DISLOCATION
FABER attitude
•Flexion, abduction, external
rotation
• Femoral head felt at groin/ scarpa
triangle/ femoral triangle
• Lengthening of limb
• Femoral vessel / femoral nerve
injury
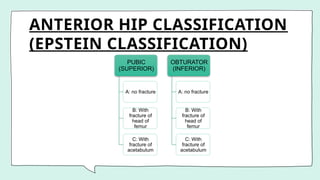
ANTERIOR HIP CLASSIFICATION
(EPSTEINCLASSIFICATION)
PUBIC
(SUPERIOR)
A: no fracture
B: With
fracture of
head of
femur
C: With
fracture of
acetabulum
OBTURATOR
(INFERIOR)
A: no fracture
B: With
fracture of
head of
femur
C: With
fracture of
acetabulum
53.
• Posterior dislocationof hip is most commonly associated with Posterior wall
acetabular fracture
• Anterior hip dislocation is commonly associated with impaction fractures of femoral
head
• CENTRAL DISLOCATION : Medial position of femoral head after a fracture involving
medial wall of acetabulum of varying type.
54.
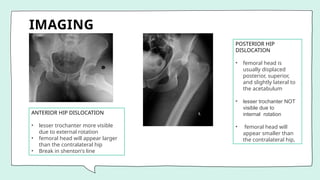
IMAGING
ANTERIOR HIP DISLOCATION
•lesser trochanter more visible
due to external rotation
• femoral head will appear larger
than the contralateral hip
• Break in shenton's line
POSTERIOR HIP
DISLOCATION
• femoral head is
usually displaced
posterior, superior,
and slightly lateral to
the acetabulum
• lesser trochanter NOT
visible due to
internal rotation
• femoral head will
appear smaller than
the contralateral hip,
55.
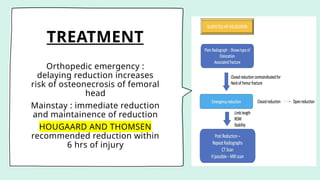
TREATMENT
Orthopedic emergency :
delayingreduction increases
risk of osteonecrosis of femoral
head
Mainstay : immediate reduction
and maintainence of reduction
HOUGAARD AND THOMSEN
recommended reduction within
6 hrs of injury
56.
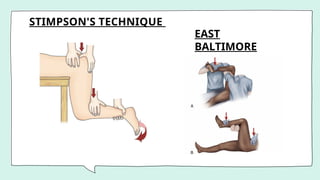
Reduction techniques
• Stimsonmethod
• Allis technique –Walker modification of Allis technique
• Bigelow
• East Baltimore Lift
• Rochester
• New – PGI Technique
57.
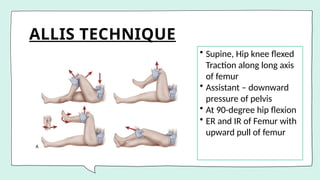
ALLIS TECHNIQUE
• Supine,Hip knee flexed
Traction along long axis
of femur
• Assistant – downward
pressure of pelvis
• At 90-degree hip flexion
• ER and IR of Femur with
upward pull of femur
58.
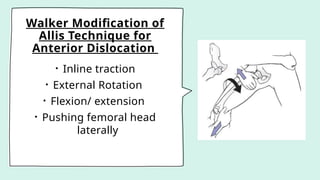
Walker Modification of
AllisTechnique for
Anterior Dislocation
• Inline traction
• External Rotation
• Flexion/ extension
• Pushing femoral head
laterally
PGI TECHNIQUE
Most atraumaticway of reducing the hip joint
• Single surgeon
• Maneuvers after sedation and anesthesia :
1a, 1b – limb is completely flexed until upper part of
thigh touches the
abdomen
1c – once complete flexion is achieved limb is
abducted as much as possible
1d – once full abduction is achieved – external
rotation is done – Click is heard and joint is
reduced
61.
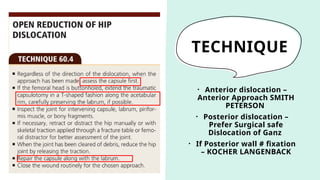
OPEN REDUCTION
INDICATION
• Irreducibledislocations(2 Closed reduction attempts failed)
• Unstable after CPR
• Intraarticular fragment post reduction
• Fracture of femur head
• Iatrogenic sciatic nerve palsy
62.
TECHNIQUE
• Anterior dislocation–
Anterior Approach SMITH
PETERSON
• Posterior dislocation –
Prefer Surgical safe
Dislocation of Ganz
• If Posterior wall # fixation
– KOCHER LANGENBACK
63.
AFTER REDUCTION
post reduction
•Check limb length
• Check range of motion
• Check for stability
• Knee and hip flexed 90 degree
• If hip remains stable , Adduction and
IR + posterior force
Most literature suggest - no need
for skeletal or skin traction post
reduction
• Range of motion exercises from
Day 1
• Weight bearing mobilization as
tolerated
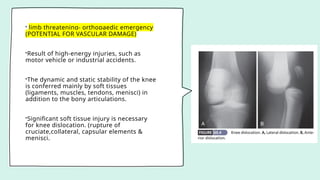
• limb threatening-orthopaedic emergency
(POTENTIAL FOR VASCULAR DAMAGE)
•Result of high-energy injuries, such as
motor vehicle or industrial accidents.
•The dynamic and static stability of the knee
is conferred mainly by soft tissues
(ligaments, muscles, tendons, menisci) in
addition to the bony articulations.
•Significant soft tissue injury is necessary
for knee dislocation. (rupture of
cruciate,collateral, capsular elements &
menisci.
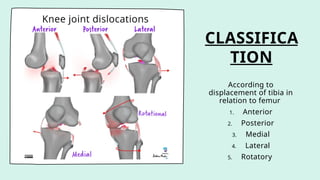
67.
MECHANISM OF INJURY
•High-energy: A motor vehicle accident with a "dashboard" injury.
• Low-energy: athletic injuries, falls in an obese patient.
• Hyperextension with or without varus/valgus leads to anterior dislocation.
• Flexion plus posterior force leads to posterior dislocation (dashboard injury).
• Associated injuries include fractures of the femur, acetabulum, and tibial plateau
Clinical
presentation
• Gross kneedistortion
• Immediate reduction to be done without
waiting for radiography
• careful neurovascular examination is
critical:
• Vascular injury-popliteal artery disruption
• Nerve injuries occur in 16 to 43% of
dislocations
70.
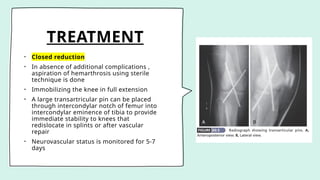
TREATMENT
• Closed reduction
•In absence of additional complications ,
aspiration of hemarthrosis using sterile
technique is done
• Immobilizing the knee in full extension
• A large transartricular pin can be placed
through intercondylar notch of femur into
intercondylar eminence of tibia to provide
immediate stability to knees that
redislocate in splints or after vascular
repair
• Neurovascular status is monitored for 5-7
days
71.
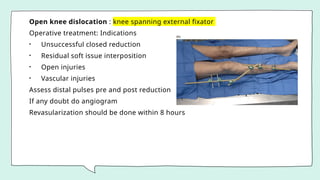
Open knee dislocation: knee spanning external fixator
Operative treatment: Indications
• Unsuccessful closed reduction
• Residual soft issue interposition
• Open injuries
• Vascular injuries
Assess distal pulses pre and post reduction
If any doubt do angiogram
Revasularization should be done within 8 hours
OTHER
DISLOCATIONS
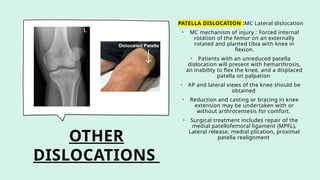
PATELLA DISLOCATION :MCLateral dislocation
• MC mechanism of injury : Forced internal
rotation of the femur on an externally
rotated and planted tibia with knee in
flexion.
• Patients with an unreduced patella
dislocation will present with hemarthrosis,
an inability to flex the knee, and a displaced
patella on palpation
• AP and lateral views of the knee should be
obtained
• Reduction and casting or bracing in knee
extension may be undertaken with or
without arthrocentesis for comfort.
• Surgical treatment includes repair of the
medial patellofemoral ligament (MPFL),
Lateral release, medial plication, proximal
patella realignment
74.
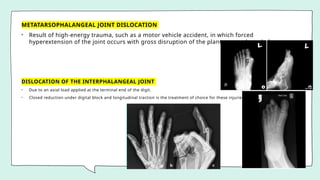
METATARSOPHALANGEAL JOINT DISLOCATION
•Result of high-energy trauma, such as a motor vehicle accident, in which forced
hyperextension of the joint occurs with gross disruption of the plantar capsule and plate.
DISLOCATION OF THE INTERPHALANGEAL JOINT
• Due to an axial load applied at the terminal end of the digit.
• Closed reduction under digital block and longitudinal traction is the treatment of choice for these injuries.
75.
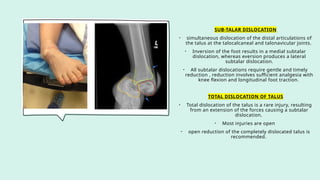
SUB-TALAR DISLOCATION
• simultaneousdislocation of the distal articulations of
the talus at the talocalcaneal and talonavicular joints.
• Inversion of the foot results in a medial subtalar
dislocation, whereas eversion produces a lateral
subtalar dislocation.
• All subtalar dislocations require gentle and timely
reduction , reduction involves sufficient analgesia with
knee flexion and longitudinal foot traction.
TOTAL DISLOCATION OF TALUS
• Total dislocation of the talus is a rare injury, resulting
from an extension of the forces causing a subtalar
dislocation.
• Most injuries are open
• open reduction of the completely dislocated talus is
recommended.
76.
LUNATE DISLOCATION
High energyinjuries to the wrist associated with neurological
injury and poor functional outcomes
occurs when wrist extended and ulnarly deviated
Treatment closed reduction and casting
If fails open reduction, ligament repair, fixation, possible
carpal tunnel release.
METACARPOPHALANGEAL JOINT DISLOCATION
• Dorsal dislocations are the most common.
• Simple dislocations are reducible and present with a
hyperextension posture.
•Reduction can be achieved with initial hyperextension followed
by distal translation and simple flexion of the joint
77.
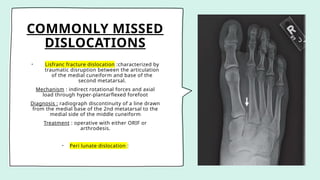
COMMONLY MISSED
DISLOCATIONS
• Lisfrancfracture dislocation :characterized by
traumatic disruption between the articulation
of the medial cuneiform and base of the
second metatarsal.
Mechanism : indirect rotational forces and axial
load through hyper-plantarflexed forefoot
Diagnosis : radiograph discontinuity of a line drawn
from the medial base of the 2nd metatarsal to the
medial side of the middle cuneiform
Treatment : operative with either ORIF or
arthrodesis.
• Peri lunate dislocation :
78.
References
• Campbell's operativeorthopaedics (14th edition )
• Rockwood and green's fracture in adults (5th edition)
• Varshnay's essential orthopaedics (3rd edition)
• Handbook of fracture by kenneth Egol ,kenneth J koval (1st SAE)
• www.google.com (image search)
Editor's Notes
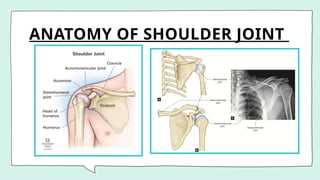
#9 The shoulder girdle is composed of three bones (clavicle, scapula, and proximal humerus) and four articular surfaces (sternoclavicular [SC], acromioclavicular [AC], glenohumeral, and scapulothoracic)