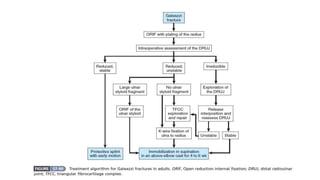
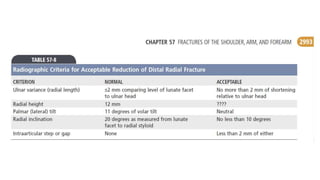
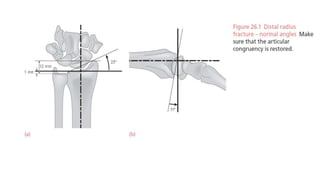
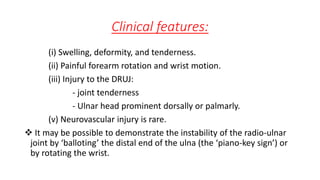
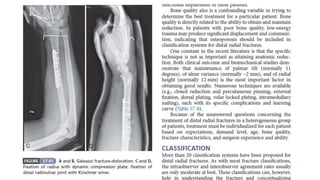
This document discusses Galeazzi fracture dislocations, which involve a fracture of the distal or middle third of the radius shaft combined with dislocation of the distal radioulnar joint. It describes the typical mechanism of injury, importance of recognizing these injuries, anatomy and functions of the triangular fibrocartilage complex, radiographic evaluation, clinical features, and treatment approaches including closed or open reduction and internal fixation followed by immobilization to stabilize the reduced distal radioulnar joint. Complications are also outlined.





































![FOREARM_FRACTURES[1].pptx and management](https://cdn.slidesharecdn.com/ss_thumbnails/forearmfractures1-250813120934-75e3f6d7-thumbnail.jpg?width=640&height=640&fit=bounds)




















































