Downloaded 70 times

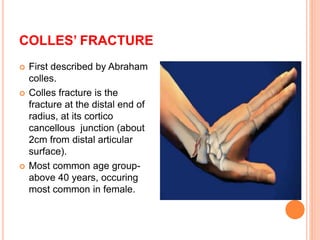









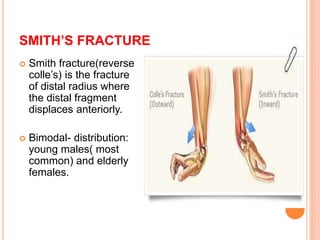
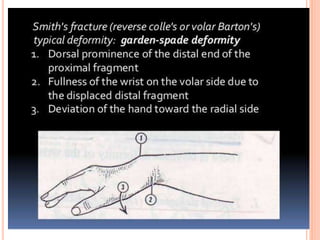



















This document summarizes several types of fractures that can occur in the forearm and wrist as a result of falling onto an outstretched hand. It describes Colles' fracture, which is the most common and involves a break in the radius near the wrist. It also discusses Smith's fracture, which is a reverse Colles' fracture with the distal fragment displaced anteriorly. Other fractures mentioned include Monteggia, Galeazzi, scaphoid, and supracondylar fractures of the humerus. For each type, the document outlines the mechanism of injury, clinical features, diagnosis using x-rays, and treatment approaches.







































![FOREARM_FRACTURES[1].pptx and management](https://cdn.slidesharecdn.com/ss_thumbnails/forearmfractures1-250813120934-75e3f6d7-thumbnail.jpg?width=640&height=640&fit=bounds)

































