Downloaded 36 times




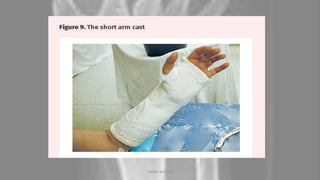
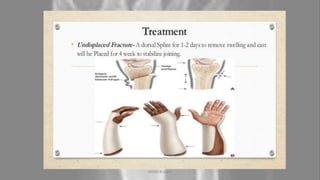


The Colles' fracture is a break of the radius bone close to the wrist that results in an upward displacement of the bone. It is typically caused by falling on an outstretched hand. Treatment depends on the severity but may include casting, closed reduction, open reduction and internal fixation. Physiotherapy focuses on regaining range of motion and strength through exercises over several phases of rehabilitation. Prevention includes proper nutrition, exercise, and wrist protection.












































































