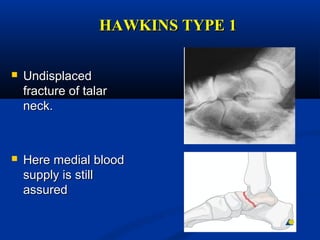
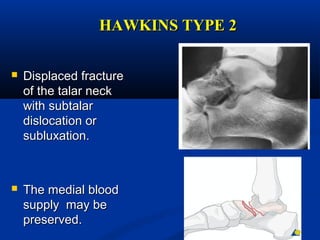
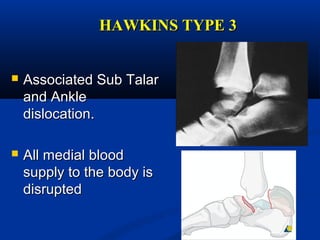
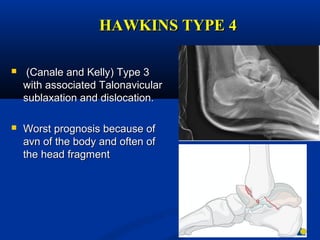
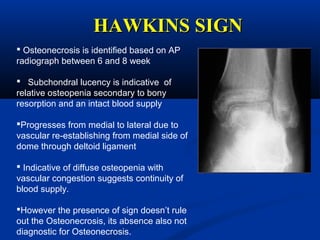
Fractures of the talus can be classified based on their anatomical location. Fractures of the talar neck are further classified using the Hawkins classification system which grades the fractures based on the displacement of the talar body. Hawkins type I fractures are undisplaced while types II-IV involve increasing degrees of displacement including subtalar dislocation. Treatment depends on the fracture type with nondisplaced fractures typically treated non-operatively and displaced fractures requiring surgical reduction and fixation to restore anatomy and avoid complications.