This document provides information on scaphoid fractures and perilunate dislocations of the wrist. It begins with an introduction to scaphoid fractures, including their incidence and location. It then describes the anatomy of the scaphoid bone and its articulations. Mechanisms of injury are explained as hyperextension injuries. Classification systems for scaphoid fractures and perilunate dislocations are outlined. Clinical assessment, investigations including imaging, complications, and types of perilunate dislocations are summarized.
Posterolateral corner injuries of knee joint Samir Dwidmuthe
Missed posterolateral corner injuries of knee joint is a common cause for failure of ACL and PCL reconstruction only next to malpositioned tunnels.
Isolated PLC injuries are uncommon, making up <2% of all acute knee ligamentous injuries. Covey JBJS 2001
Incidence of PLC injuries associated with concomitant ACL and PCL disruptions are much more common (43% to 80%). Ranawat JAAOS 2008
A recent (MRI) analysis of surgical tibialplateau fractures demonstrated an incidence of PLC injuries in 68% of cases. Gardner JOT 2005
Take home message
PLC injuries to be ruled out in every case of ACL& PCL rupture.
Neurovascular integrity to be checked in every case.
Grade I & II can be managed conservatively.
Grade III Acute- Repair.
Grade III Chronic- Anatomic PLC recon.
Beware of varus knee alignment.
Deformity: It’s the position of a limb/Joint, from which it cannot be brought back to its normal anatomical position.
Described as abnormalities of :
Length
Angulation
Rotation
Translation
Combination
Posterolateral corner injuries of knee joint Samir Dwidmuthe
Missed posterolateral corner injuries of knee joint is a common cause for failure of ACL and PCL reconstruction only next to malpositioned tunnels.
Isolated PLC injuries are uncommon, making up <2% of all acute knee ligamentous injuries. Covey JBJS 2001
Incidence of PLC injuries associated with concomitant ACL and PCL disruptions are much more common (43% to 80%). Ranawat JAAOS 2008
A recent (MRI) analysis of surgical tibialplateau fractures demonstrated an incidence of PLC injuries in 68% of cases. Gardner JOT 2005
Take home message
PLC injuries to be ruled out in every case of ACL& PCL rupture.
Neurovascular integrity to be checked in every case.
Grade I & II can be managed conservatively.
Grade III Acute- Repair.
Grade III Chronic- Anatomic PLC recon.
Beware of varus knee alignment.
Deformity: It’s the position of a limb/Joint, from which it cannot be brought back to its normal anatomical position.
Described as abnormalities of :
Length
Angulation
Rotation
Translation
Combination
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
2. INTRODUCTION
➢ First described by Cousin & Destot in 1889
-Position of the scaphoid on the radial side of the wrist,
as the proximal extension of the thumb ray, makes it vulnerable
to injury.
Incidence:
➢ 10-15% of the hand and wrist fractures.
➢ It’s the most frequently fractured carpal bone around 70%
➢ Of these 70% occurs in waist.
4. ◈ Derived from greek word “skaphos” meaning boat
◈ Boat or cashew shaped bone
◈ Parts of the scaphoid:
proximal pole
waist
distal pole
tubercle
5. ◈ Small irregular S shaped tubular bone, located at
a 45degree plane to the longitudinal &
horizontal axes of the wrist.
◈ Since its 80% of its surface is articular cartilage,
reduced capacity for periosteal reaction &
increased tendency for delayed & non union.
◈ Distal pole is pronated, flexed & ulnarly
angulated with respect to the proximal pole.
6. ◈ ARTICULATIONS: with 5 bones
Proximal surface- radius
Distal surface- split into two separate articular surfaces by a
bony ridge & laterally with trapezoid & trapezium, medially with
capitate
Ulnar surface- lunate
7. ◈ ATTACHMENTS:
- No musculotendinous attachments
Ligamentous
Extrinsic ligaments are
-radioscaphocapitate
-radioscapholunate
-radial collateral ligament
Intrinsic ligaments are
-scaphotrapezium-trapezoid
-scaphocapitate ligament
-scapholunate ligament
8. Blood supply
✓ Retrograde blood supply via two vascular pedicles
✓ Originating from the scaphoid branches of the
radial artery
✓ Dorsal branch
-70 to 80% (proximal part)
-enters via small foramina present along the
spiral groove & dorsal ridge
✓ Volar branch
-20 to 30% (distal scaphoid)
-enters via the scaphoid tubercle
Note-minimal or no perforating vasculature at waist
10. Hyperextension injury
Fall on outstretched hand
Wrist is dorsiflexed to>95degrees
& radially deviated to >10
degrees
Compression occurs dorsally and
tension on palmar surface of
wrist
Bending forces applied to waist and distal pole of
scaphoid as proximal pole is tightly held between
the capitate, dorsal lip of radius and taut palmar
capsule
Leads to fracture
scaphoid most
commonly waist
11. ➢ Degree of force and position of the wrist at the time of injury –
determines the type & severity
➢ Herbert suggested that wrist deviation may predict the location of
the fracture as the line of midcarpal joint crosses the
proximal pole -in radial deviation
distal pole -in ulnar deviation
➢ Waist # -usually due to shear forces
➢ Tubercle # - either compression or avulsion
➢ Waist -60-70%
➢ Proximal 3rd
-25%
➢ Distal 3rd
-10%
14. AO classification- based on anatomic location
Scaphoid(72)
Non comminuted(72.A) Comminuted(72.B)
proximal pole(72.A1) 72.B1
waist (72.A2) 72.B2
distal pole(72.A3) 72.B3
Russe classification-based on inclination of the fracture line
Horizontal
oblique
Vertical(unstable)
15. Mayo classification (based on location & stability)
based on location-5 types
Unstable fracture:
o >1mm of # displacement
o Lateral intrascaphoid angle>35 degrees
o Bone loss or comminution
o Fracture malalignment
o Proximal pole #
o perilunate # dislocation
17. ➢ Diagnosis made by combination of clinical history,
examination & radiographic assessment.
➢ History of hyperextension to wrist following a fall,
sports ,RTA or punch injury
Clinical Symptoms:
Radial sided wrist pain following a fall onto
the outstretched hand, with almost 90% recalling the
hyperextension injury
Swelling
ecchymosis(rarely)
19. Scaphoid shift test( Watson test)
◈ Pressure applied over the
tubercle & wrist moving
from radial to ulnar
deviation
◈ Positive test- if there is a
“clunk” as the scaphoid
subluxes dorsally out of
the scaphoid fossa
◈ Inference –
scapholunate disruption
20. ◈ Reduced thumb
movement
◈ Anatomical snuff box
swelling
◈ Anatomical snuff box
pain in ulnar deviation
◈ Pain on thumb/index
pinch
23. X-ray
➢ Neutral PA and lateral view:
-to assess the carpal alignment & determining the clear #
-often poor for scaphoid # detection due to tubercle overhang
on PA view and overlap on the lateral view
Ulnar deviated PA view: (scaphoid view)
-to detect the proximal pole fractures
-scaphoid fat pad is best visualized
-ulnar deviation rotates the scaphoid
parallel to the long axis of the foream and to
achieve an en face image
24. 45 degree ulnar oblique view:
-in semipronated position
-to detect tubercle fracture,Oblique sulcus
and waist(displaced)
45 degree radial oblique view:
-in semisupinated position
-to detect proximal pole #, humpback
deformity and avulsion fracture
Note-30 to 40% scaphoid # not visualised on initial
assessment & investigation with four view
radiographs
25. Ziter view:
-PA view of the wrist in ulnar deviation with 20 degree
tube angulation to the elbow
-To detect waist fracture as beam at right angles to long
axis
Soft tissue signs:
@Scaphoid fat pad sign-distortion or loss of
adjacent fat stripes over the radial aspect of the
scaphoid on the PA view
@Pronator fat pad sign- a prominent pronator
quadratus fat pad over the volar aspect of the wrist
on the lateral view
26. ➢ Barton suggested 3 possible reasons why
standard scaphoid radiographs are often
misinterpreted
- Dark line may be formed by the dorsal lip of
the radius overlapping the scaphoid
- White line formed by the proximal end of
the scaphoid tuberosity
- Dorsal ridge of the scaphoid may appear
bent on the semisupinated view
➢ Contralateral wrist views - because of the wide range of
normal alignment
27. Bone
scan-scintigraphy-Fast and reliable diagnostic tool
-100% sensitivity
Demerits-
Lacks specificity
Little information regarding location
Ultrasound:
-Inter observer variability
-Useful in patients with cortical irregularity and
hemarthrosis
-Little information on structural integrity of
scaphoid
28. CT SCAN & MRI
◈ For surgical planning & assessment of healing
◈ To diagnose additional bony & ligament injuries
Fracture displacement
step>1mm at dorsal cortices
gap > 1mm in sagittal or coronal views
◈ To measure the scaphoid fracture displacement-3 angles
-Lateral intrascaphoid angle measurement
-Normal 30+/-5degrees,saggital view
>35* -cut off for displacement.
-angle created by lines drawn perpendicular
to the proximal & distal articular surfaces/poles
29. ◈ Dorsal cortical angle (sagittal view)
-Normal-140 degrees;
-Abnormal >160*
-Angle created by tangential lines drawn along the dorsal
cortices of
proximal & distal scaphoid fragments
Scaphoid height to length ratio (sagittal view)
-normal 0.60, abnormal->0.65
-length is determined by a palmar line drawn from the most
proximal to
the most distal edge
-height is the maximal point with a line perpendicular to the
length line
31. Malunion
-Humpback deformity (proximal scaphoid rotates dorsally into
extension & distal part faces downward in flexion)
-Wrist pain, reduced wrist extension &diminished grip strength
-Loss of extension is proportional to the angular deformity, which is
best calculated by lateral intrascaphoid angle & height to length ratio
Humpback
deformity
32. Non union
• Leads to specific type of post traumatic wrist arthrosis
called Scaphoid nonunion advance collapse(SNAC)
• Non union rate –undisplaced waist #-10%
• Displaced waist-50%
• Risk factors: delayed diagnosis & treatment
• Leads to radiocarpal arthritis & secondary mid carpal
arthritis
• Types fibrous nonunion-seen in stable #
sclerotic nonunion-unstable #
• Two patterns of nonunion displacement
-based on fracture line relative to the dorsal apex of
scaphoid ridge
Dorsal displacement-in proximal waist#
Volar displacement-in distal waist #
33. AVN
◈ Late complication of scaphoid fracture especially those
involving proximal pole fracture
◈ Preiser disease:
Scaphoid avn without a fracture either SL ligament
injury or idiopathic
-Increasing pain and stiffness of the wrist
-Small, deformed proximal pole fragment with cystic changes
& areas of sclerosis
-MRI is useful
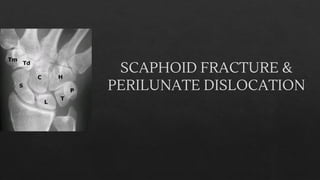
35. Perilunate dislocation & fracture
dislocation
◈ Introduction:
◈ Most common form of wrist dislocation
◈ Spectrum of injury which include both ligamentous and
osseous disruption
◈ Prefix trans –refer to associated fracture
◈ Prefix peri – dislocation
◈ Usually traumatic, high energy
◈ Occurs when wrist extended and ulnarly deviated lead to
intercarpal supination
◈ Commonly missed ~25% on initial presentation.
36. Types
◈ Greater arc injury: (perilunate fracture
dislocation)
Ligamentous injuries associated with a
fracture of one or more of the bones around the
lunate.
◈ Common pattern -transscaphoid perilunate
fracture dislocation
-Fracture neck of the capitate
-Sagittal fracture of the triquetrum
◈ Scaphocapitate syndrome:
both capitate & scaphoid fragments are
37. ◈ Lesser arc injury:
◈ Pure ligamentous injuries around the lunate
◈ Disruption of capsular & ligamentous connections of the lunate to
the adjacent carpal bones & radius without fracture
◈ Classically, the distal row dislocates in a dorsal or dorsoradial
direction
◈ SLD or LTD often persists even after relocation lead to recurrence of
instability and late carpal collapse
◈ Fracture dislocations are twice as frequent as a dislocation alone
39. Mayfield classification
◈ Progressive perilunate instability from a radial to
ulnar direction
◈ Stage 1:
◈ As the distal carpal row is violently extended
,supinated & ulnarly deviated, STT and SC
ligaments are tightened causing the scaphoid to
extend
◈ As the scaphoid extends, SL ligament transmits
the force to lunate, which can’t rotate as much as
scaphoid because its constrained by the
palmarly located radiolunate & ulnolunate
ligaments leading to scaphoid # or SLD
40. ◈ STAGE II:
◈ If the extension-supination force persists, once the
proximal row has been dislocated, transmissiom of the
force distally to capitate may lead to displacement
through the space of Poirier
◈ Space of Poirier-ligament free area b/w
radioscapholunate ligament & long radiolunate
ligament at the midcarpal joint level; an area of
potential weakness.
◈ STAGE III:
◈ If the force persists, once the capitate is displace
dorsally lunotriquetral ligament disruption will occur
41. ◈ STAGE IV:
◈ If the force continues,the dorsally displaced capitate is pulled
proximally.
◈ Pressure is applied onto the drsal aspect of lunate,forcing it to
dislocate
◈ As the palmar ligaments are much stronger than the dorsal capsule,
dislocation never involves a pure palmar displacement
◈ Note-lunate dislocation is the end stage of progressive perilunate
dislocation
42. Other classification system
◈ WITVOET & ALLIEU CLASSIFICATION:
◈ Grade I - lunate appears normally
aligned
◈ Grade II - rotated palmarly <90degrees
◈ Grade III ->90 degrees but still attached
to the radius by its palmar ligaments
◈ Grade IV –totally enucleated
43. ◈ HERZBERG et al – three stage classification
◈ Stage I - dorsal dislocation of capitate but lunate
remains in fossa
◈ Stage II A - dorsal dislocation of capitate + lunate
dislocation ,rotation <90 degrees
◈ Stage II B - dislocation of capitate+lunate ,rotation >90
degrees
44. Clinical features
◈ Often young male, high energy trauma
◈ h/o hyperextension injury
◈ Wrist pain, swelling & deformity
◈ Signs- tenderness distal to lister tubercle
◈ marked prominence of entire carpus dorsally
◈ compressive test-palpable and audible snap, click or clunk
◈ Midcarpal shift test:
◈ Pressure applied over dorsum of the capitate, wrist moving from radial
to ulnar deviation
◈ Positive-clunk presents as the lunate reduces from the palmar flexed
position
45. ◈ 1/3rd
associated with polytrauma
◈ 16% -median nerve symptoms and signs
◈ Other features- ulnar neuropathy, arterial
injury or tendon disruption
◈ Late presentations:
increasing nerve symptoms or tendon
rupture than wrist deformity because to
which patient has often become accustomed
46. Investigations
◈ Xray
◈ neutral PA and lateral view
◈ In PA view –normally the anatomic axis of forearm will pass through the
head & base of 3rd
metacarpal, capitate, radial aspect of lunate, center of the
lunate fossa of radius
◈ In lateral view-line will pass through the longitudinal axis of index finger
metacarpal, capitate, lunate and the radius with the scaphoid on an axis at a
45* angle to this line
◈ Normal joint space (b/w carpal bones, carpal & metacarpals, carpal bones
&radius)
◈ < 2mm –normal
◈ >3mm -suspected ligament disruption
◈ >5mm -diagnostic
47. Spilled tea spot sign
◈ Due to palmar rotation of the lunate & disruption of lunate –capitate
articulation
48. Piece of pie sign
◈ Triangular appearance of lunate secondary to rotation
49. Gilula lines
Arc 1- along the proximal articular surface of
proximal carpal row
Arc 2-along the distal articular surface
Arc 3-proximal cortical margins of the capitate &
hamate
Normally - smooth curves
Broken arc-diagnostic of fracture and or
dislocation
50. Scapholunate angle
◈ Angle created by the longitudinal axes
of the scaphoid and the lunate
◈ Long axis of scaphoid –is a line
tangential to the palmar convex surface
of the proximal & distal poles
◈ Long axis of lunate- line perpendicular
to the line connecting the dorsal &
palmar lips of the lunate.
◈ Normal range- 30 to 60 degrees
52. Carpal-height ratio
◈ Carpal height/length of third metacarpal
◈ Carpal height(L2) is the distance b/w the base
of 3rd
metacarpal to subchondral sclerotic line
of distal radius
◈ Normal ratio 0.5
◈ <0.45 indicates carpal collapse
◈ Alternate method - Height of capitate is used
instead of third metacarpal
53. ◈ Stress radiographs- clenched fist view
To evaluate the widening of scapholunate interval
Often performed bilaterally
◈ CT & MRI to determine the extent of lesion
◈ Arthroscopy and arthrography