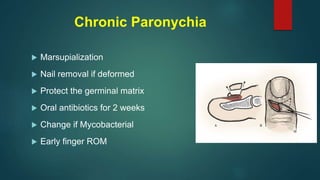
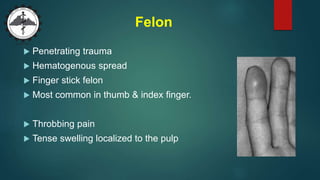
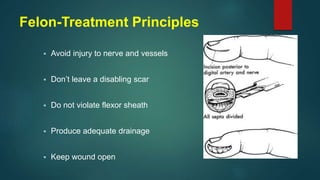
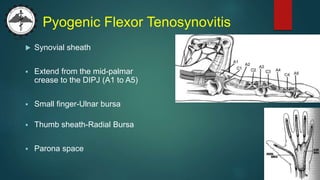
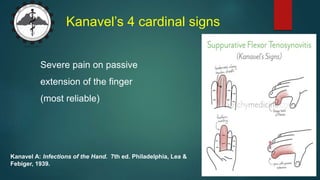
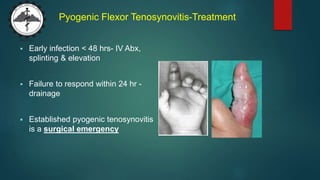
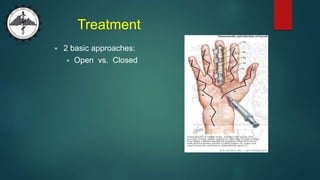
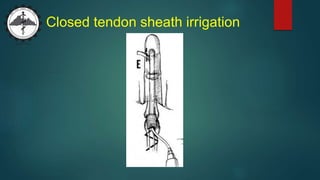
This document discusses various types of hand infections, including paronychia (infection of the nail fold), felon (deep space infection of the distal pulp), pyogenic flexor tenosynovitis (infection of the flexor tendon sheath), and deep space infections. Staphylococcus aureus is a common cause. Treatment involves antibiotics, surgical drainage if abscesses are present, splinting, and irrigation. Prompt treatment is important to prevent complications such as tendon necrosis or osteomyelitis.