Downloaded 3,023 times
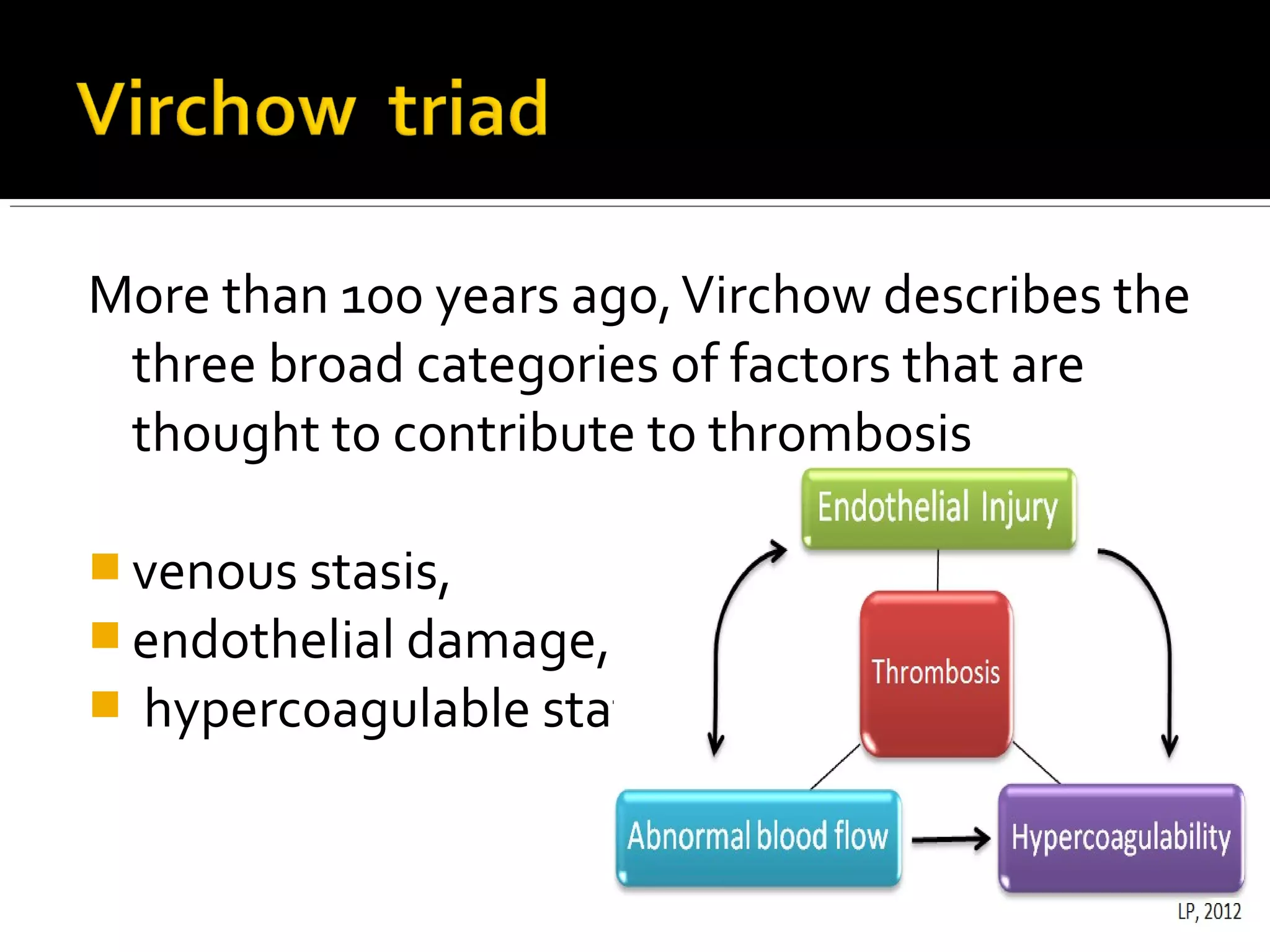






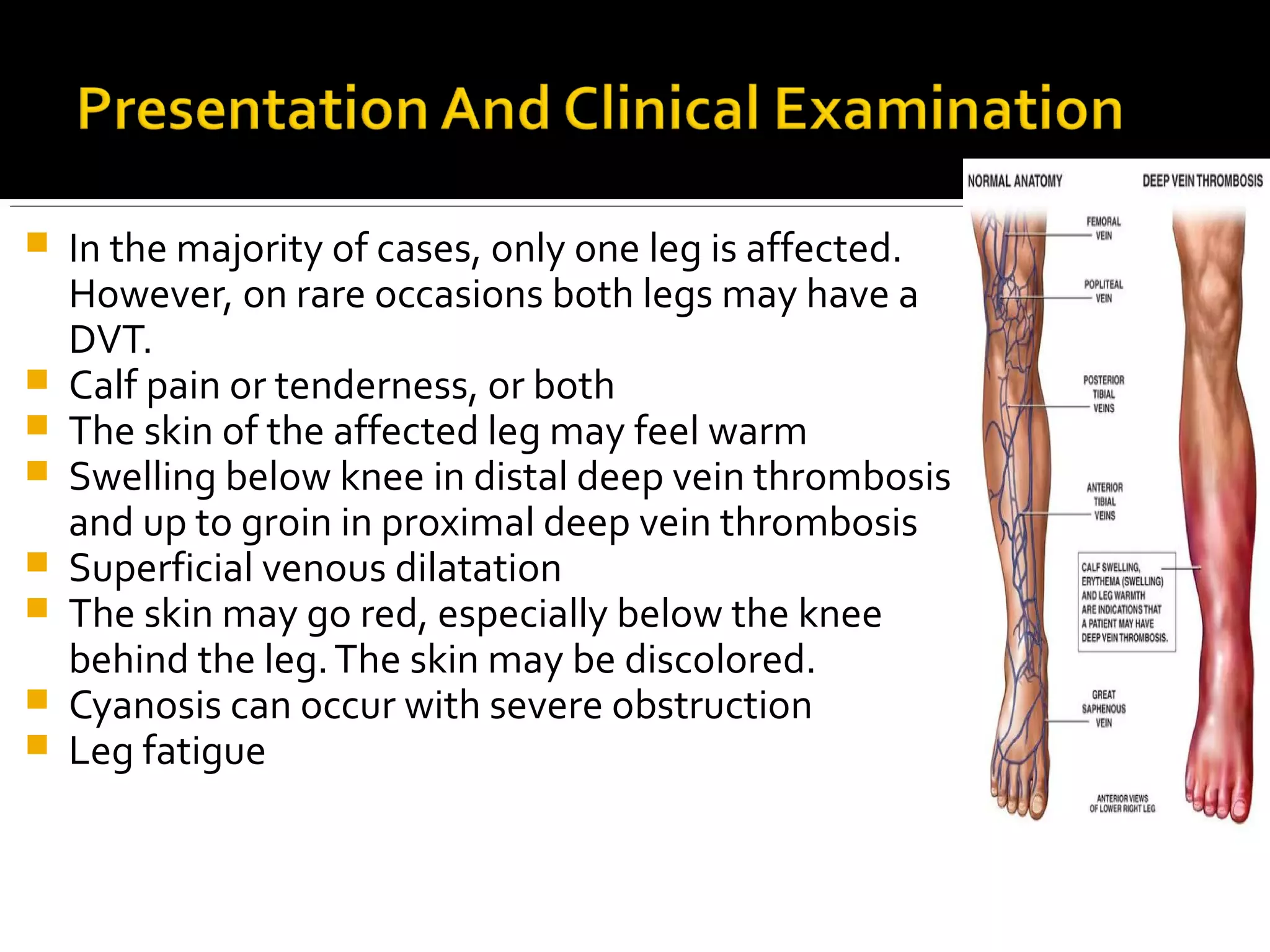



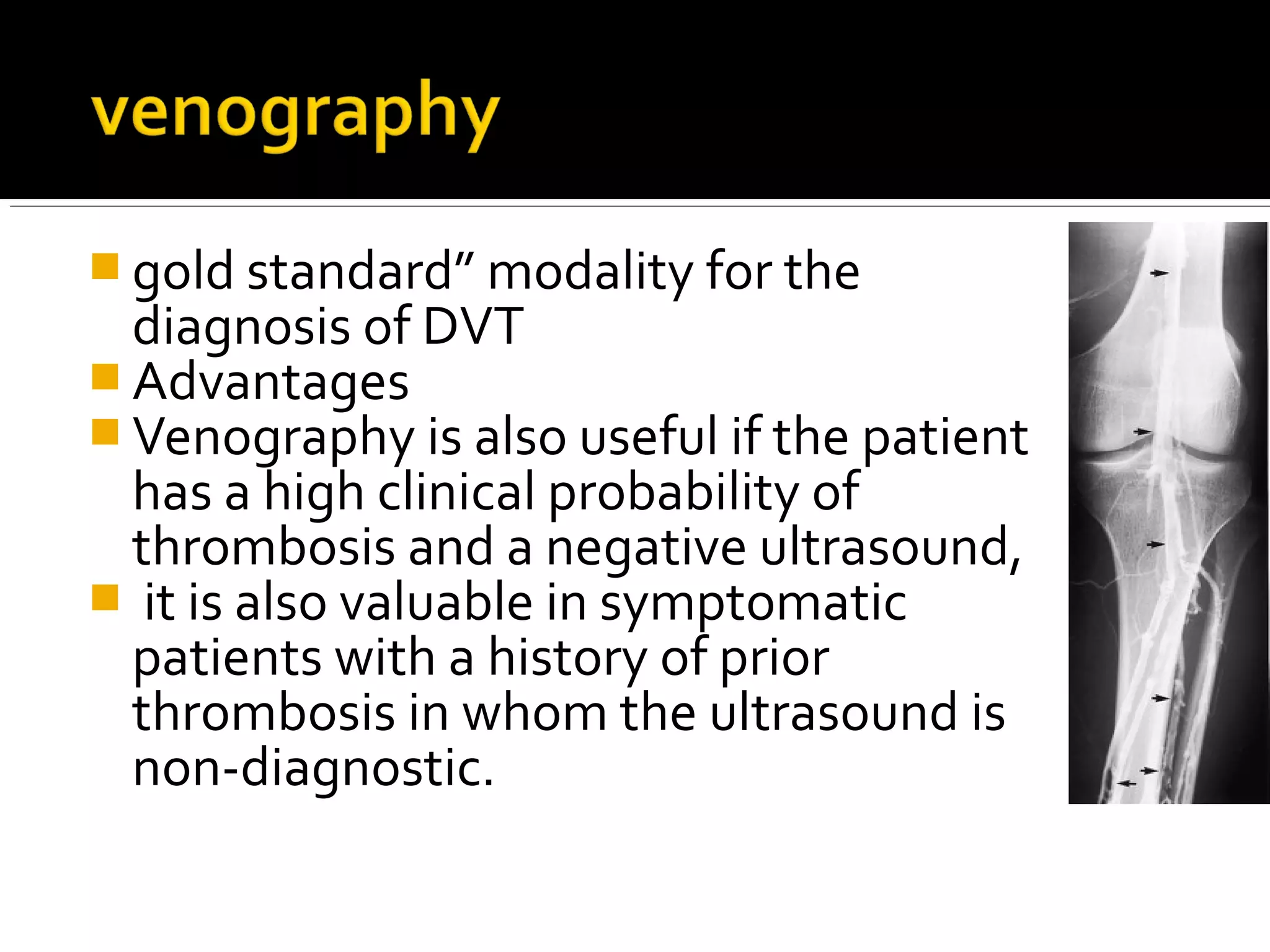



















Venous thromboembolism is a condition where a blood clot forms in a vein. Deep vein thrombosis is a blood clot that forms in deep leg veins and can dislodge and travel to the lungs, called a pulmonary embolism. Risk factors include prolonged bed rest, surgery, cancer, pregnancy, oral contraceptives, and genetic conditions. Diagnosis involves a clinical assessment, D-dimer blood test, and ultrasound or venography imaging of the legs. Treatment consists of blood thinners like heparin and warfarin to prevent further clotting and embolism.



































































