Downloaded 479 times
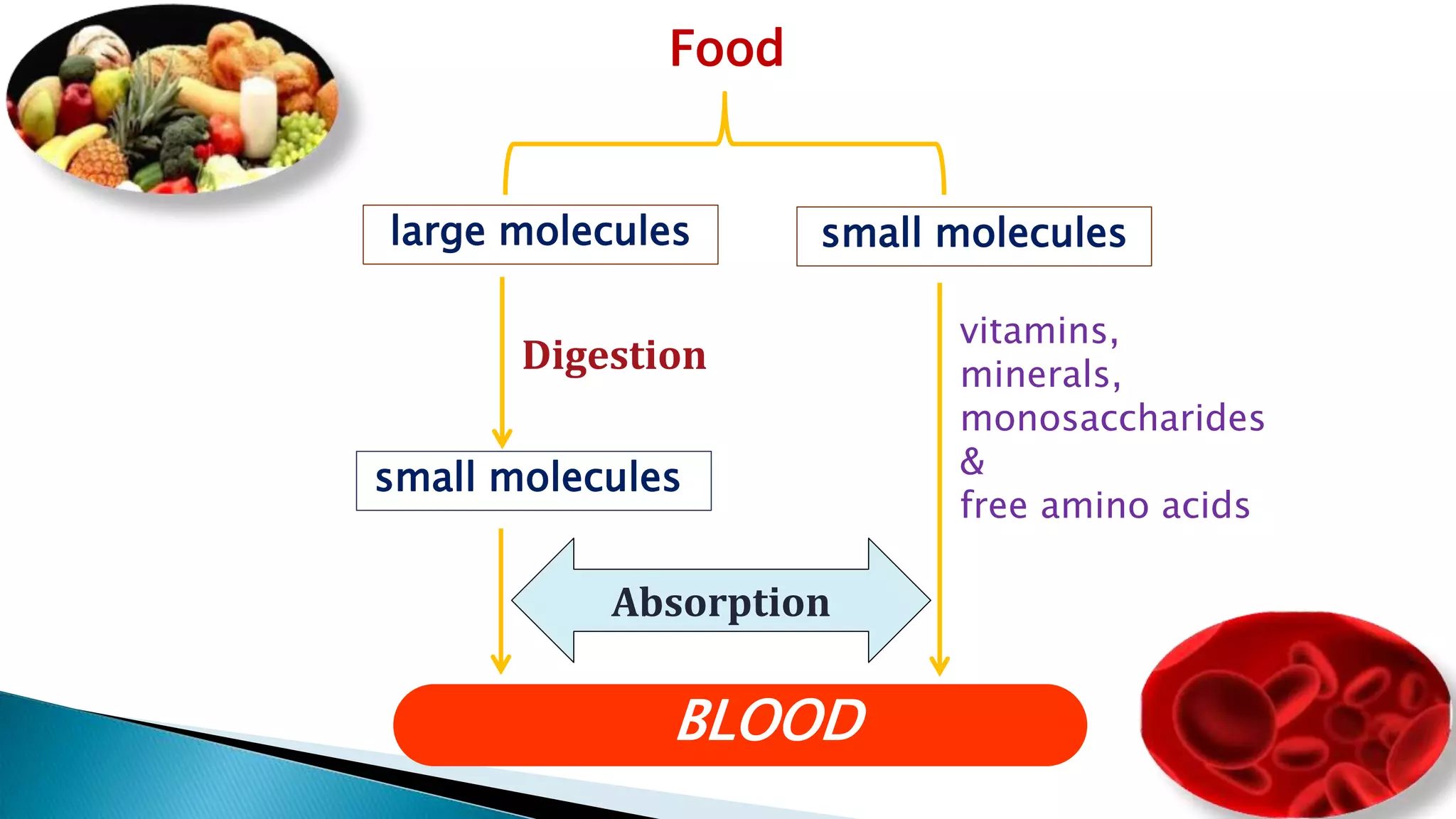
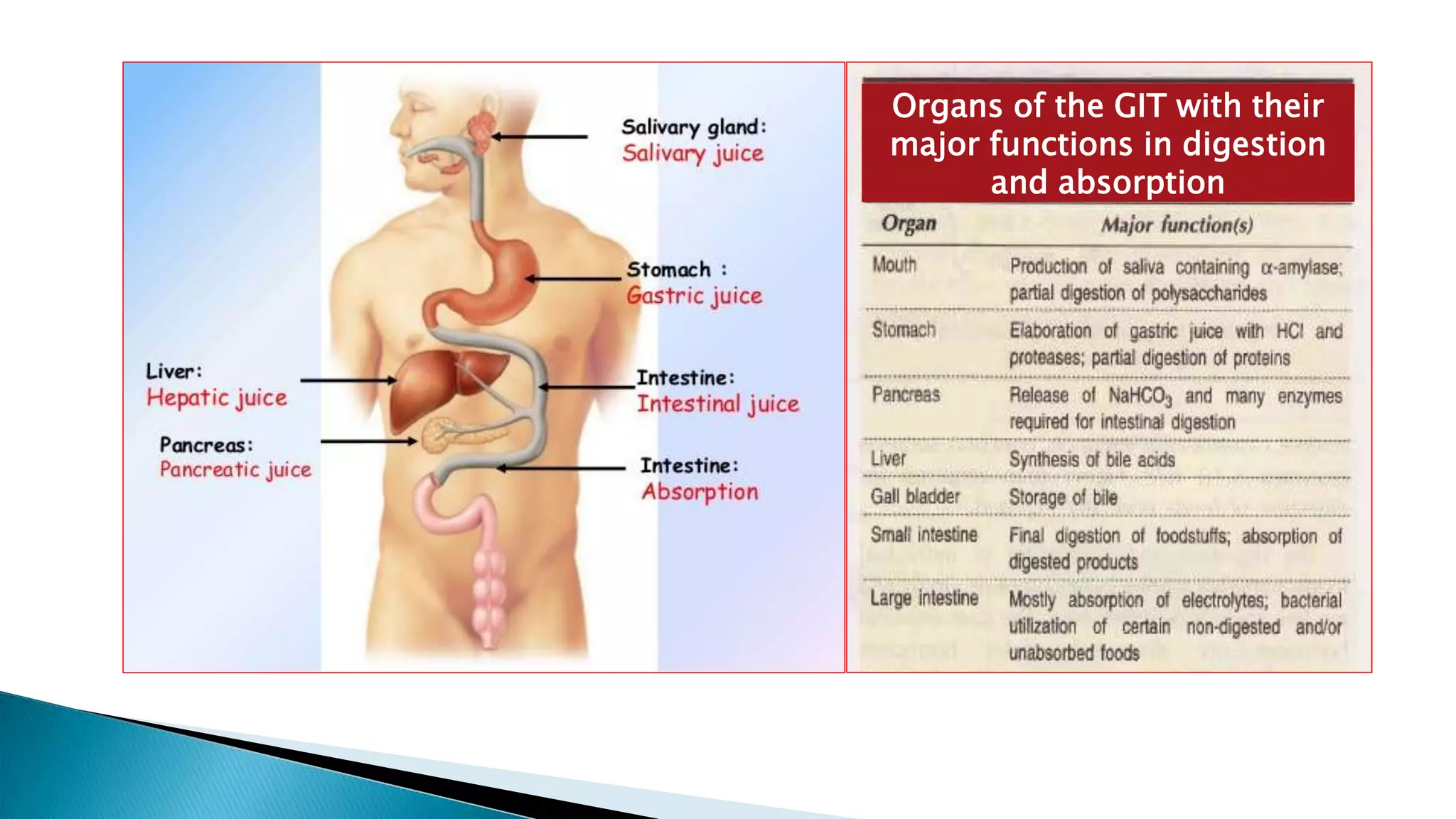
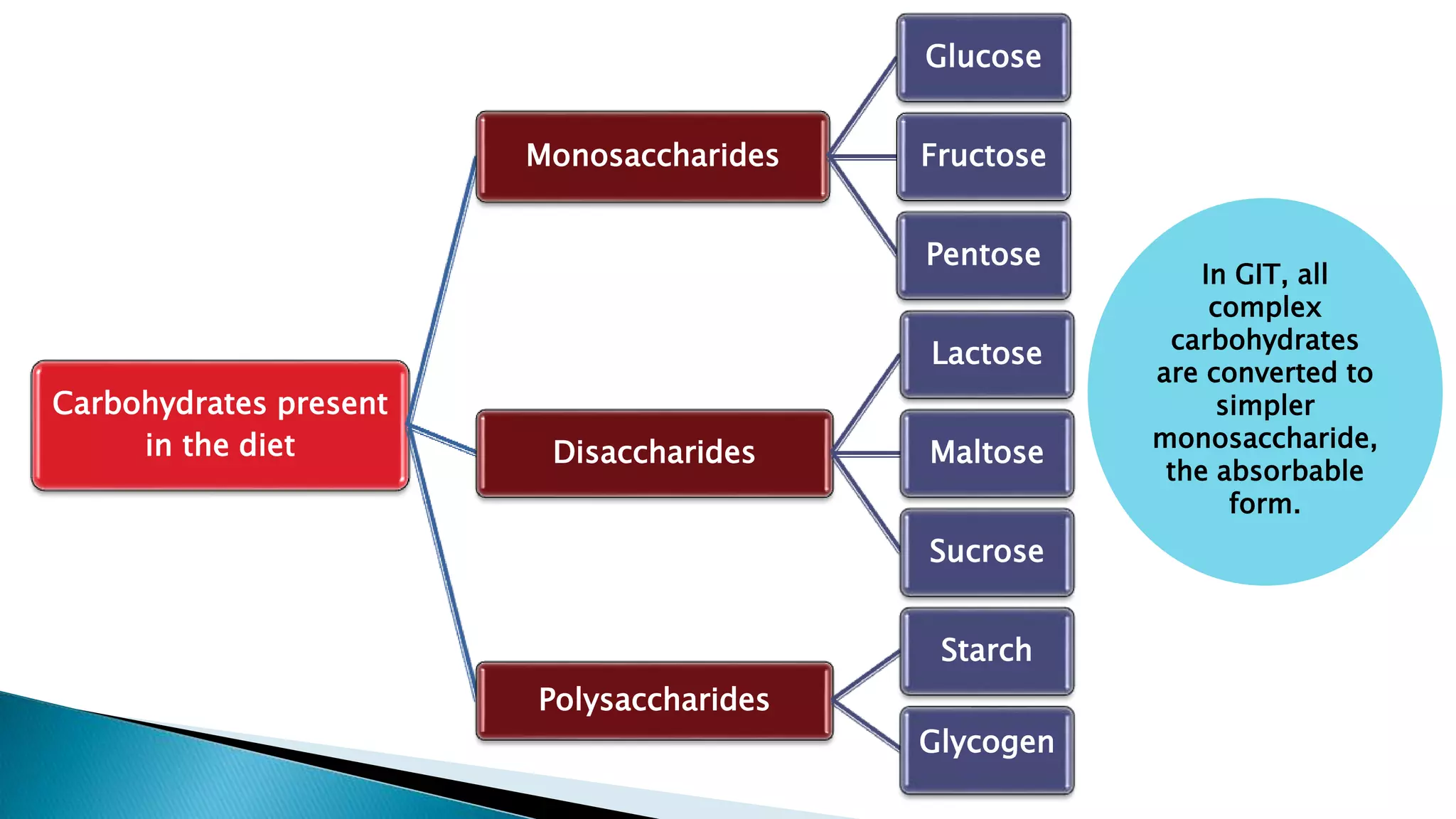
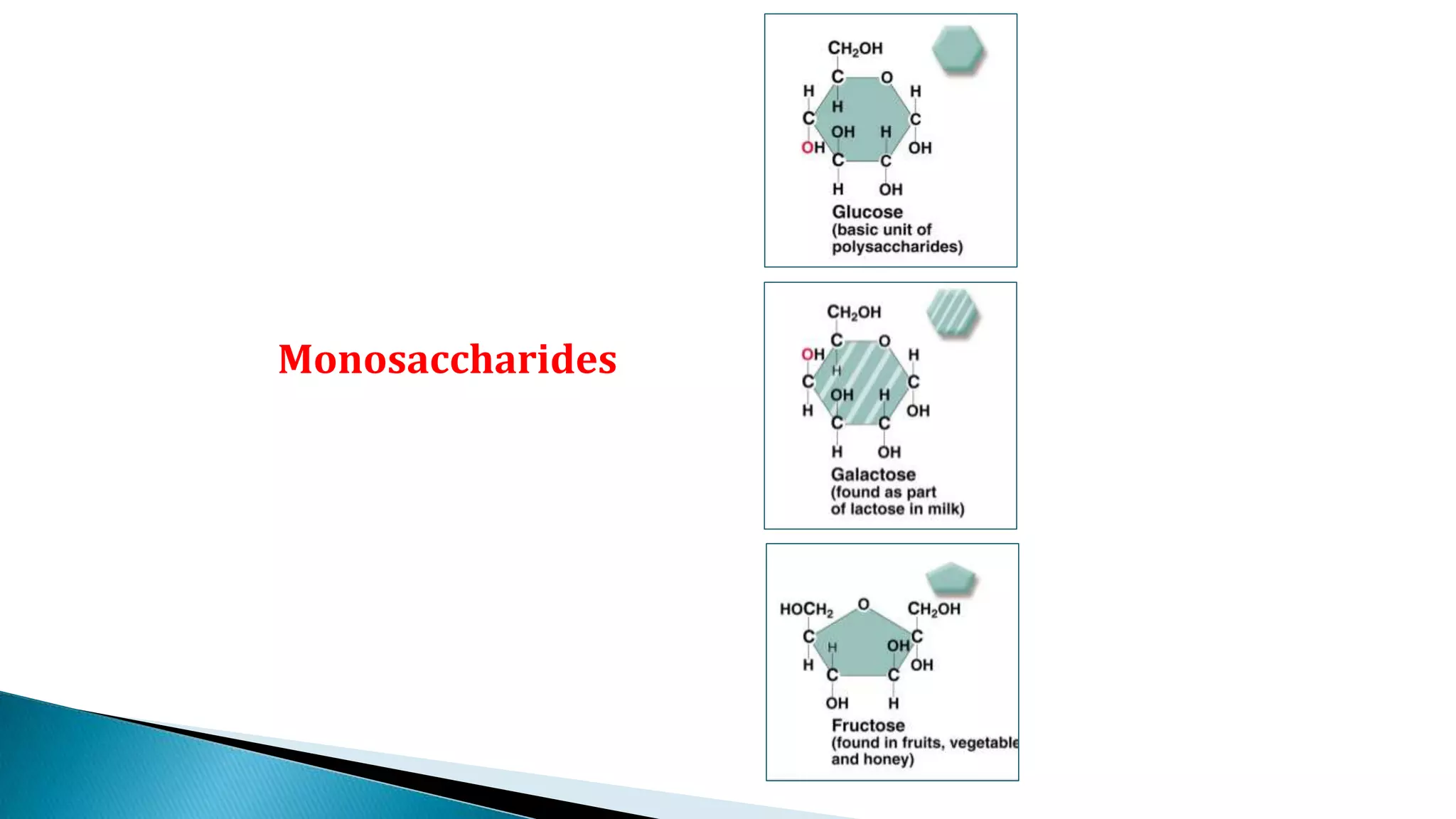
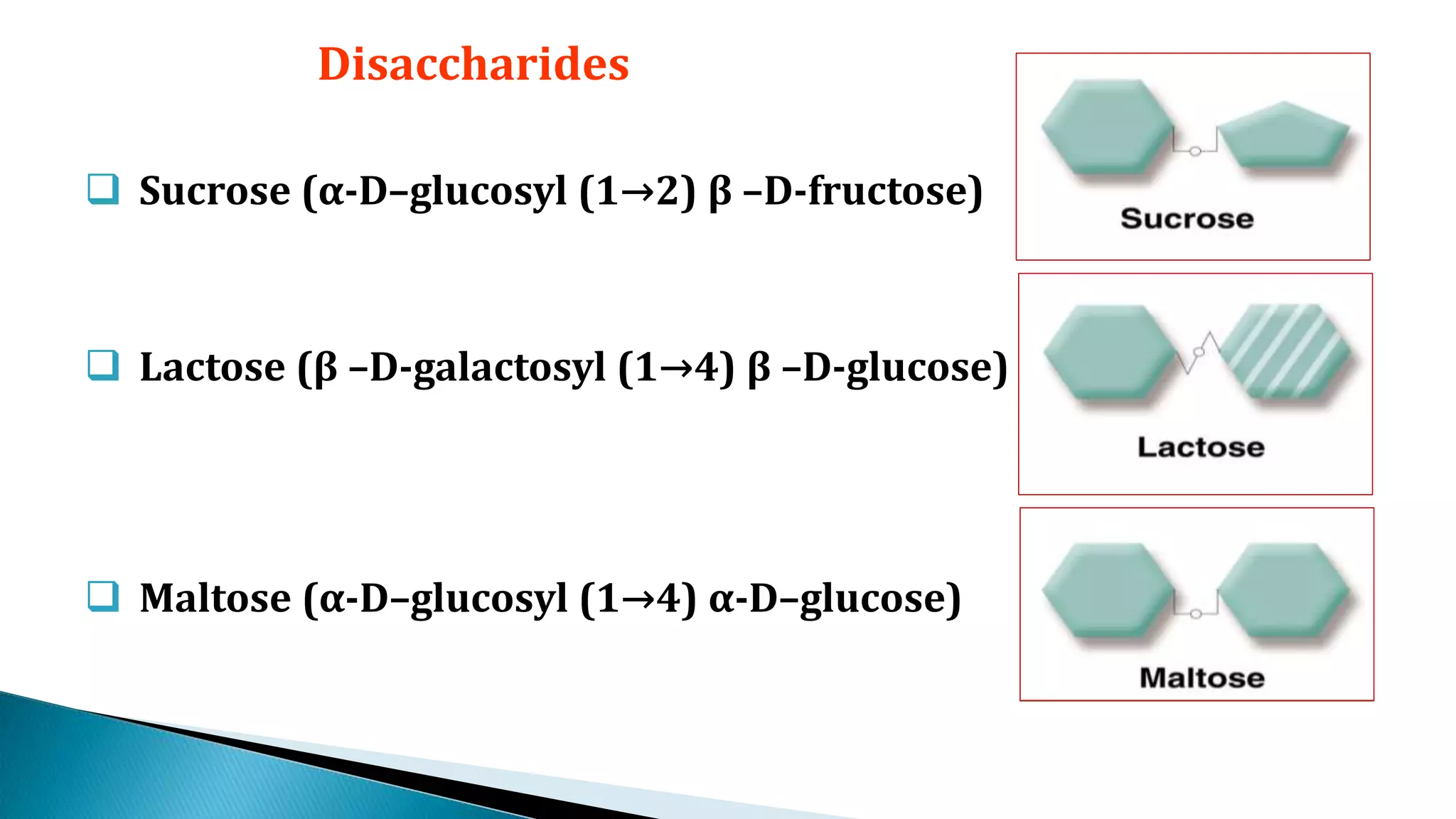
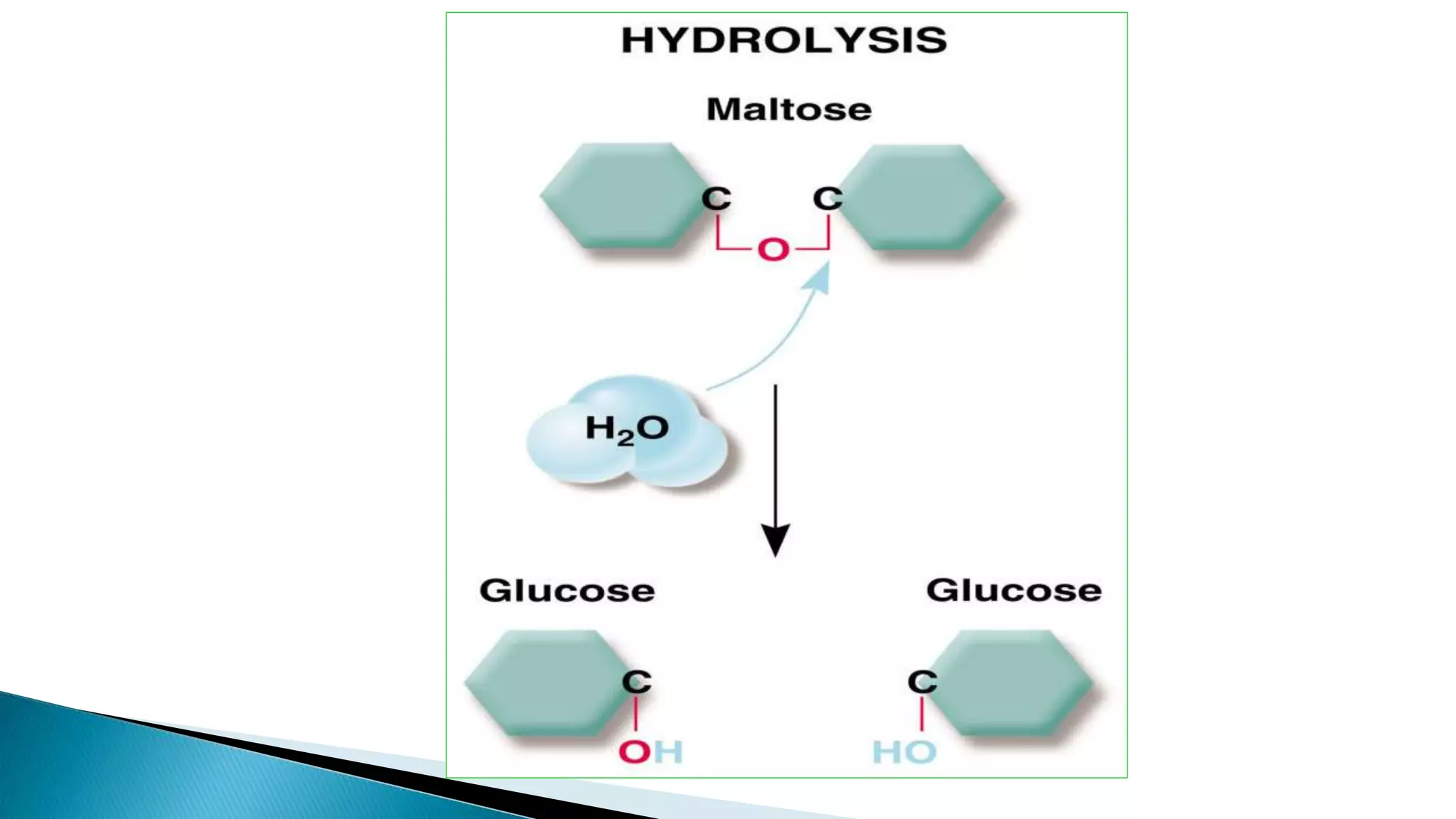
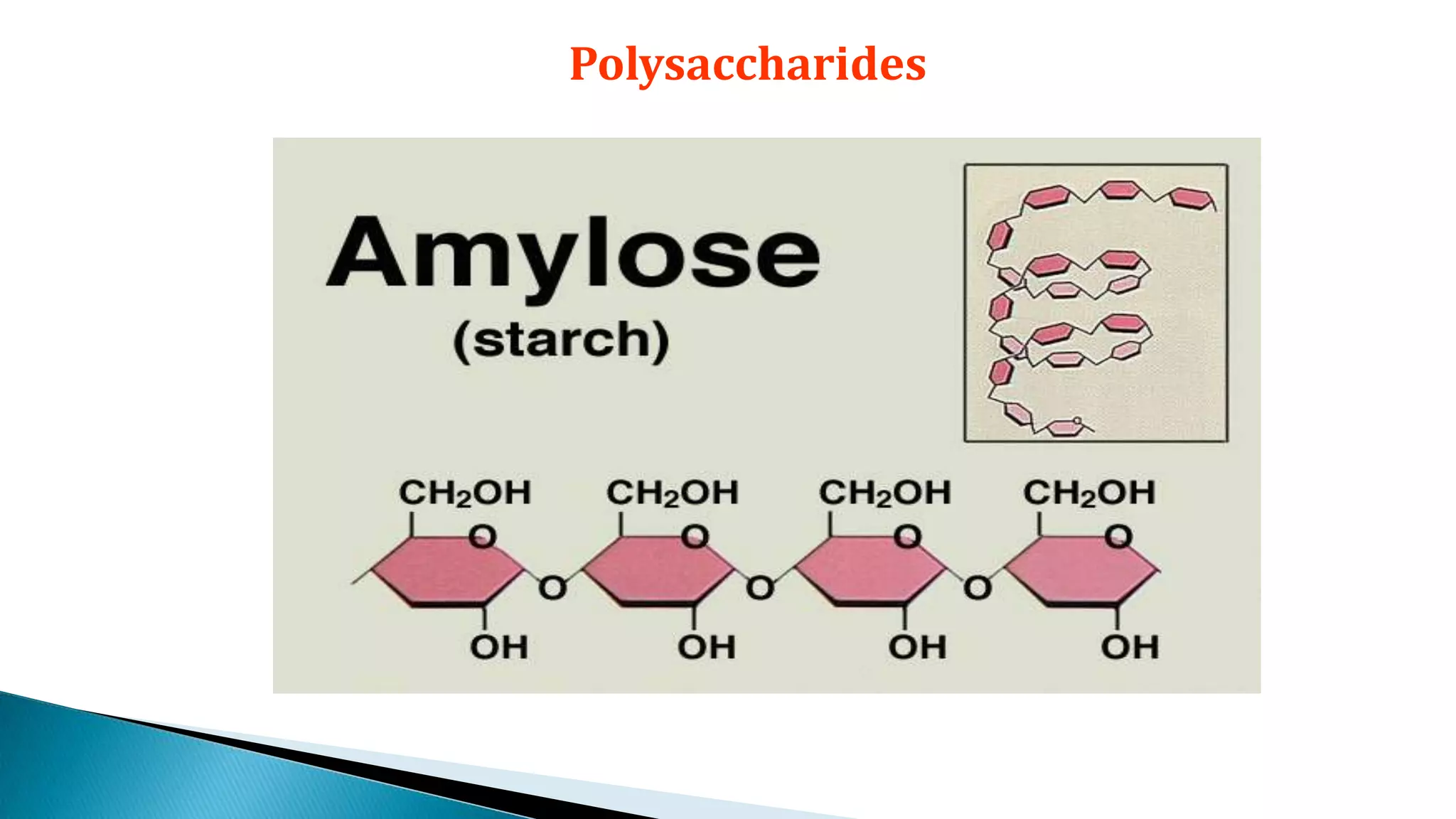
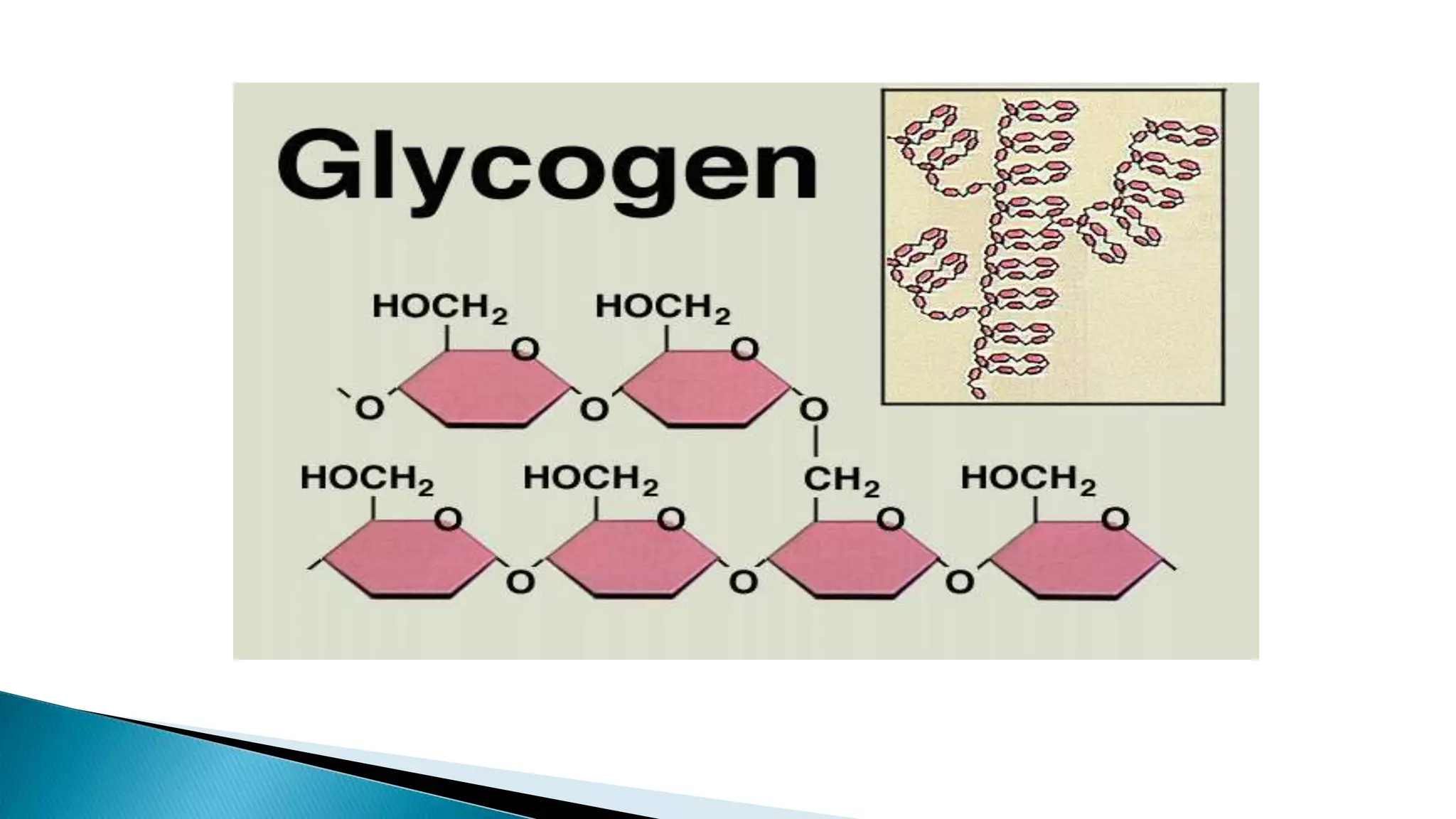
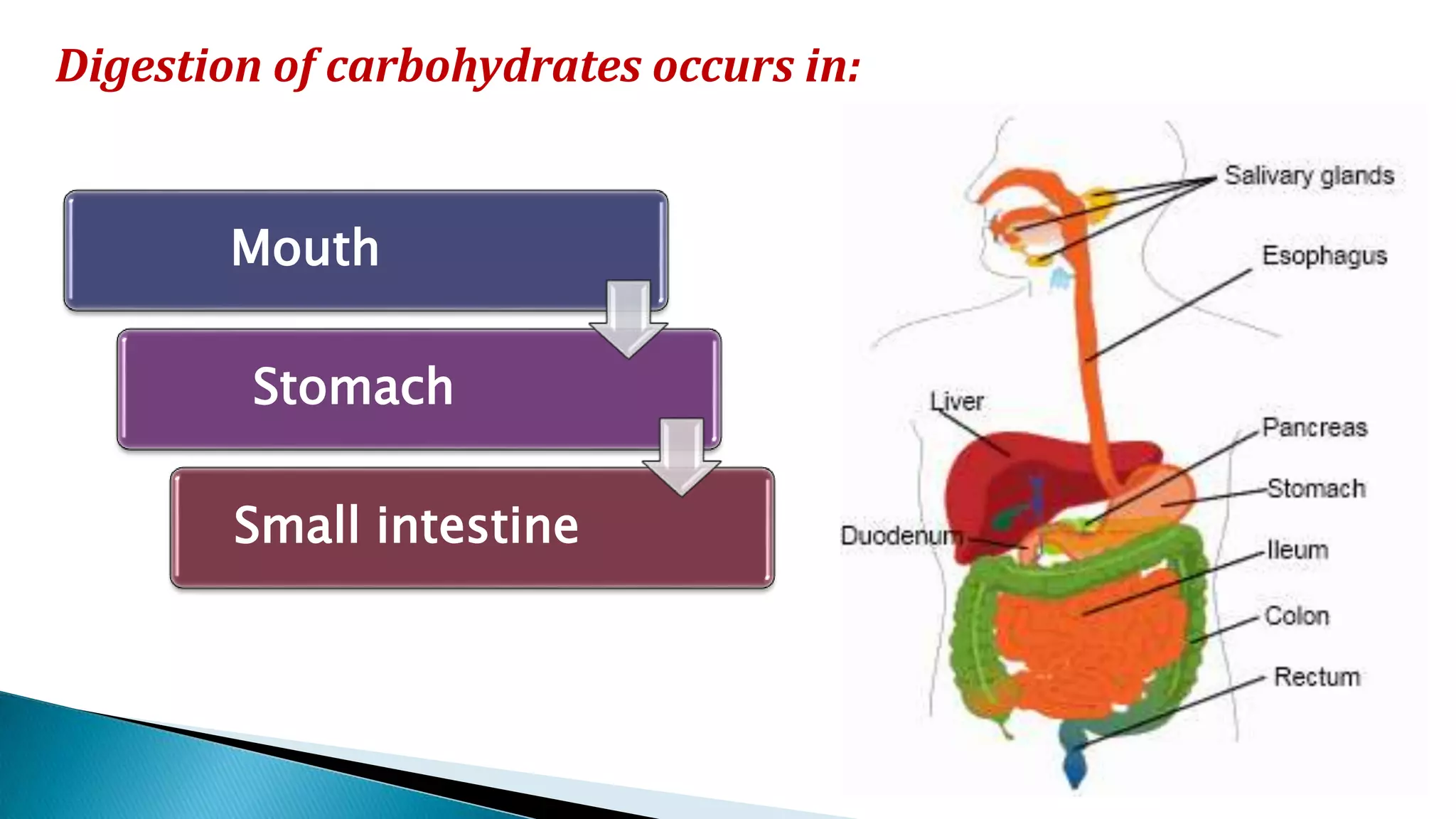
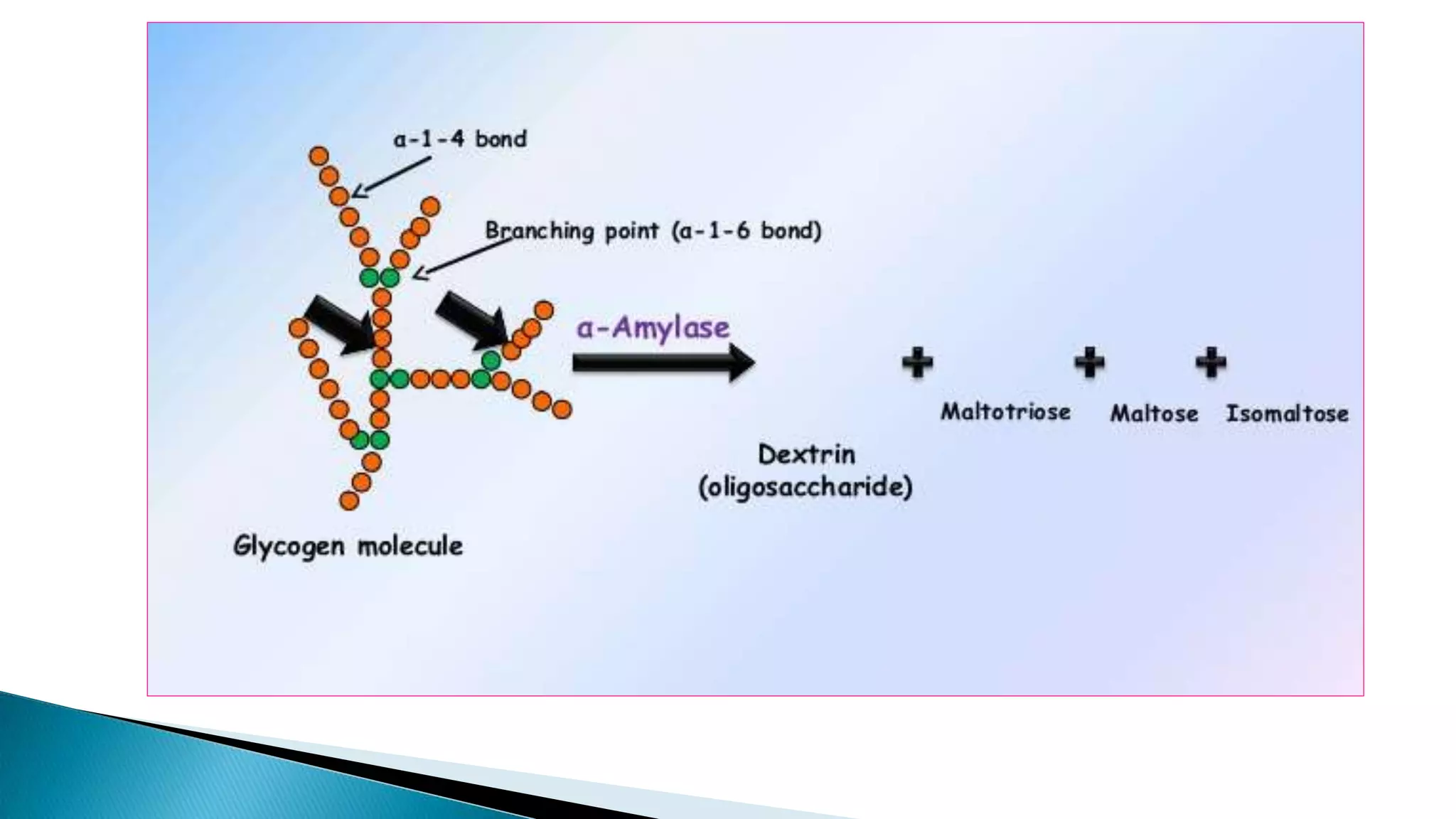
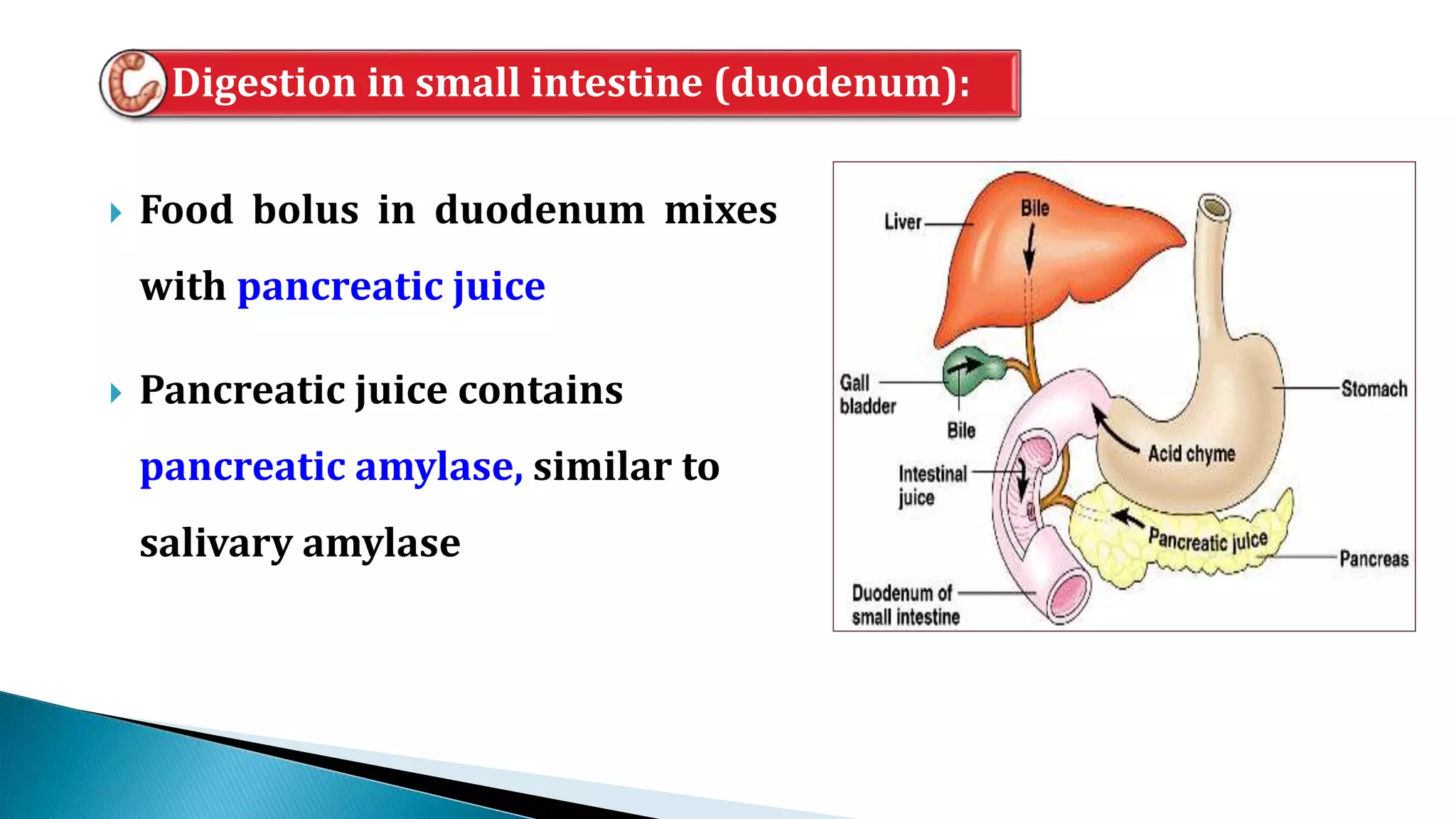
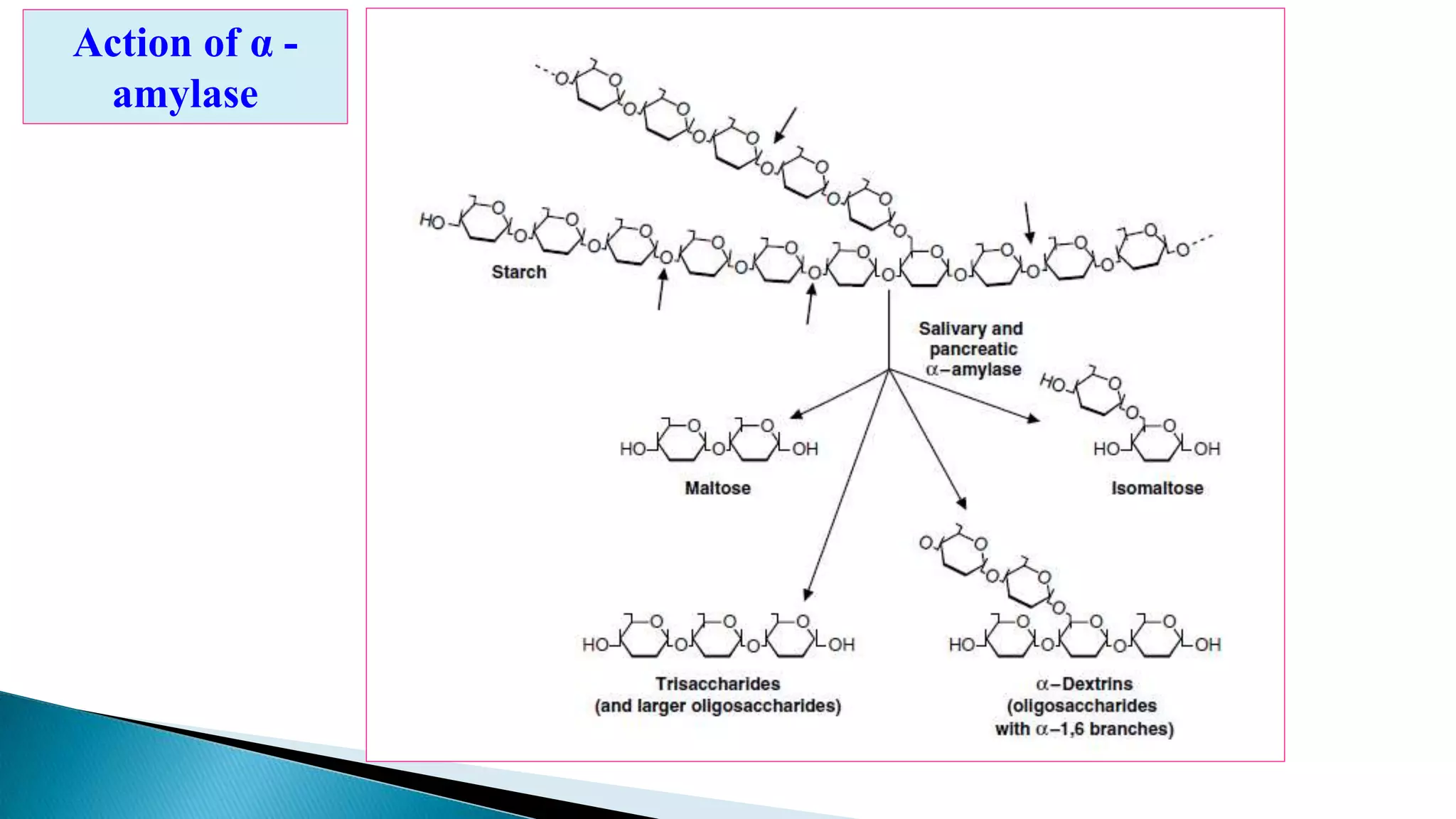

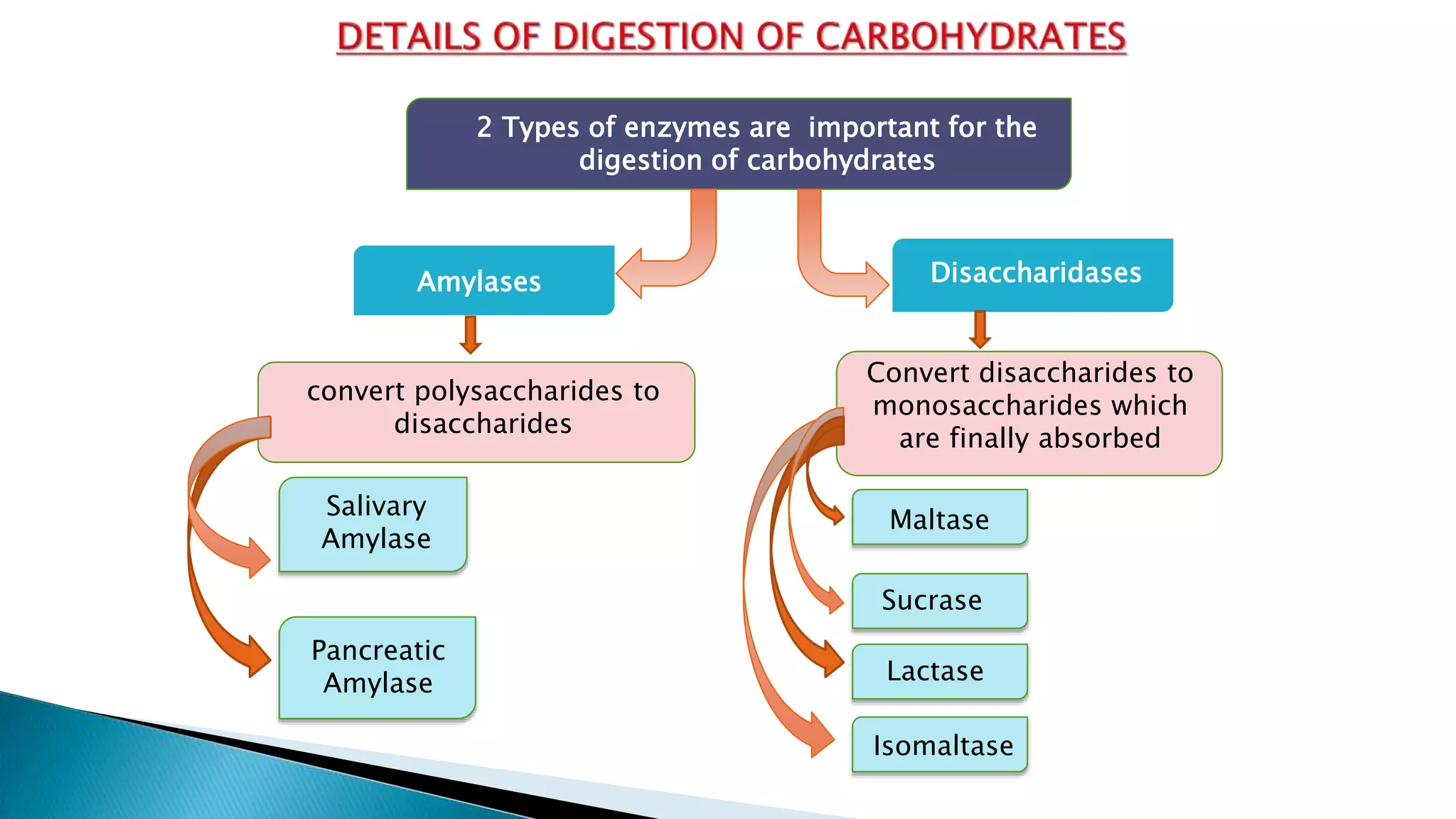





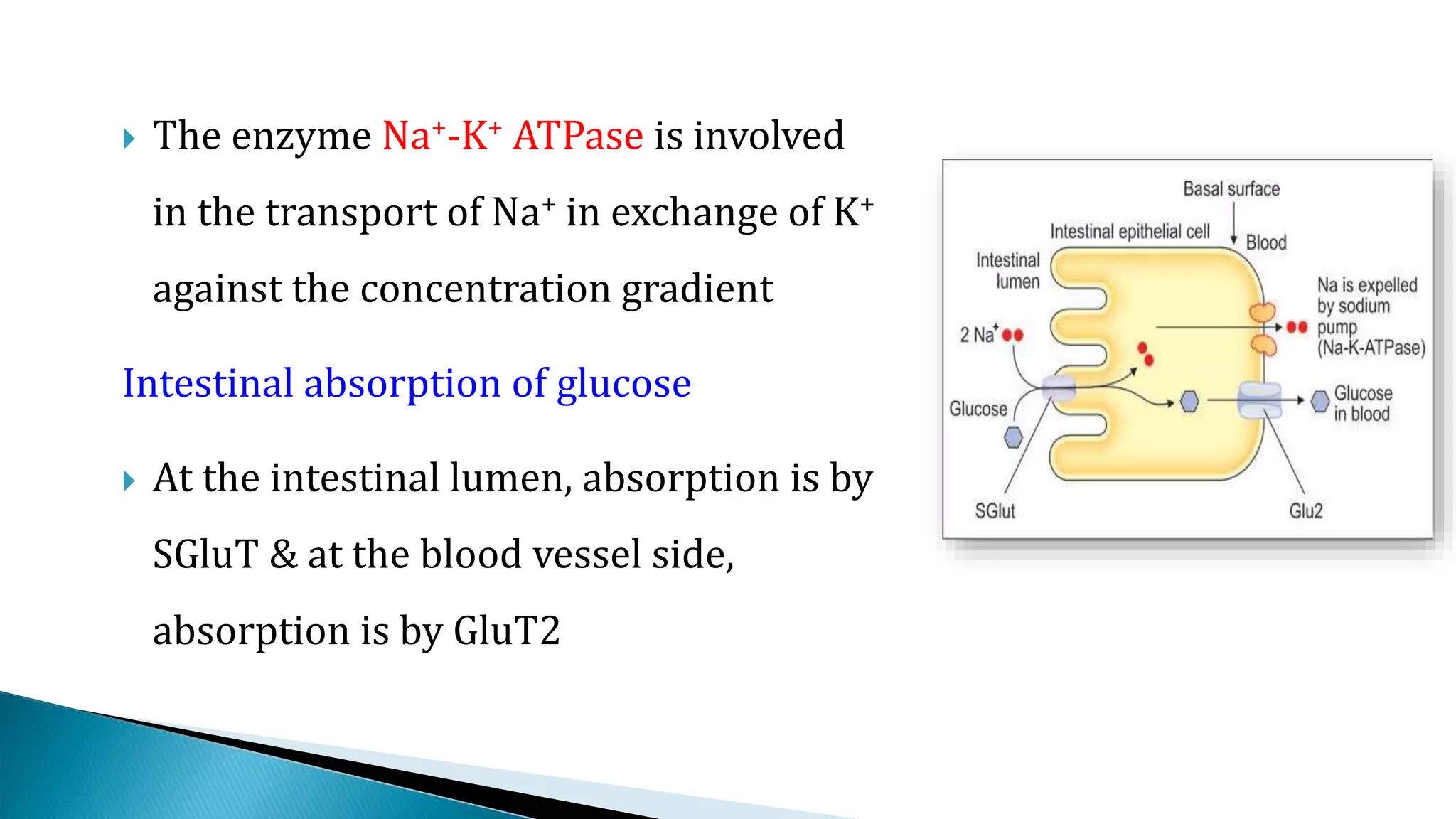






This document summarizes carbohydrate digestion in the human gastrointestinal tract. It describes how carbohydrates are broken down into smaller molecules by salivary and pancreatic amylases and intestinal disaccharidases and oligosaccharidases. The monosaccharides glucose, fructose and galactose that are produced are then absorbed into the bloodstream in the small intestine. Glucose absorption is an active process that utilizes sodium-glucose co-transporters, while fructose absorption occurs via facilitated diffusion. Factors that can influence carbohydrate absorption such as intestinal health, hormones and vitamins are also discussed.