Downloaded 1,114 times






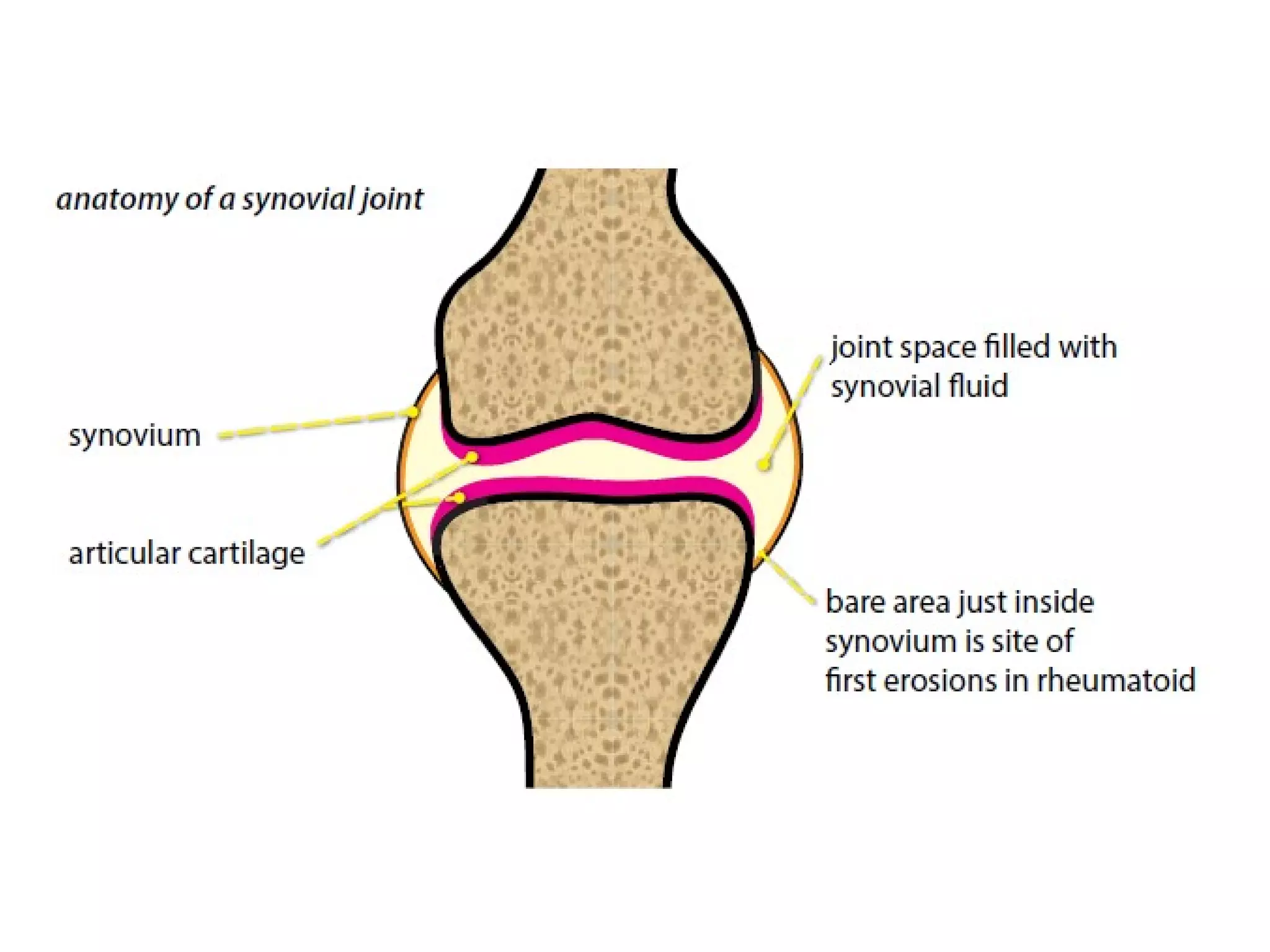


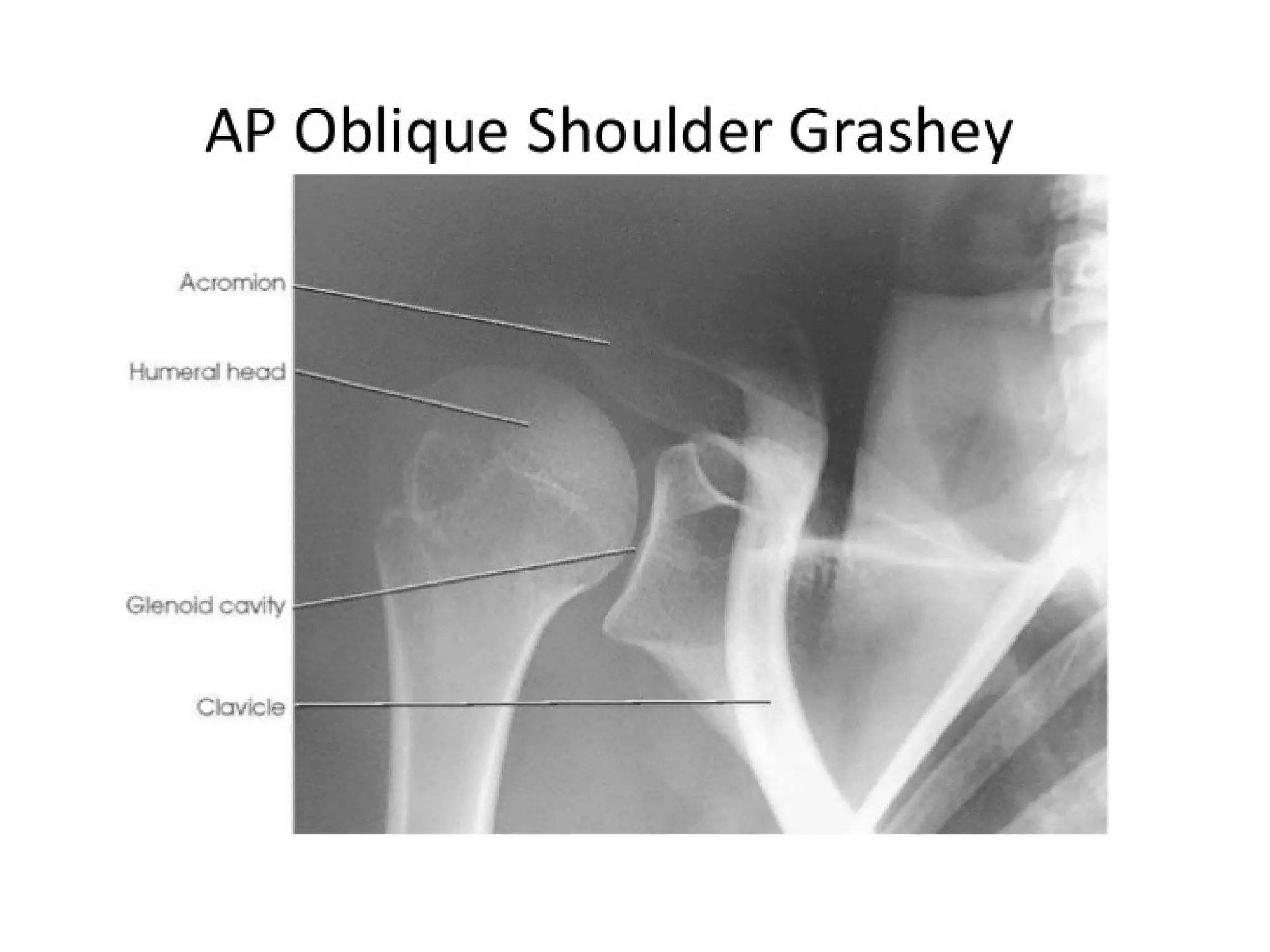





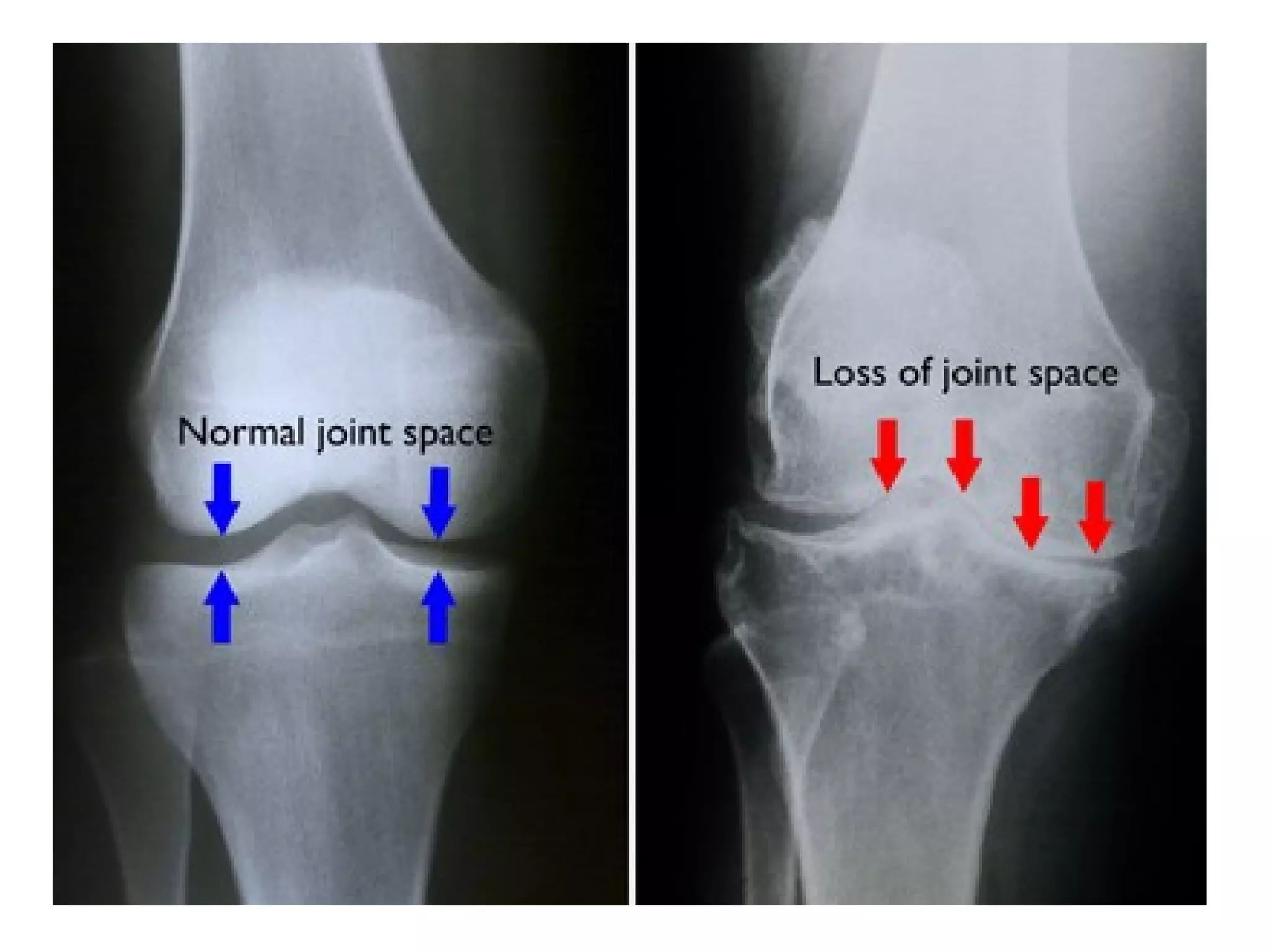

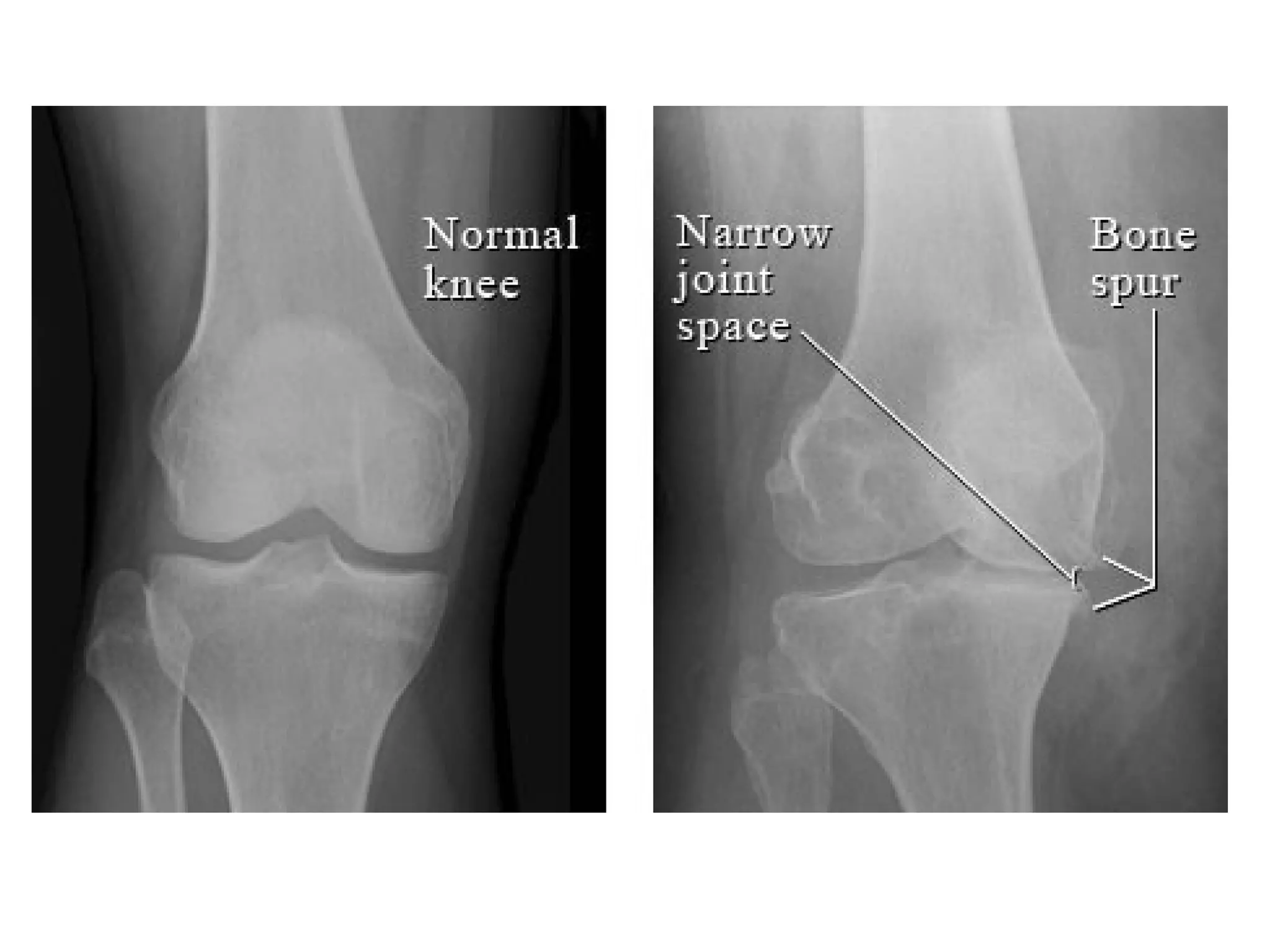



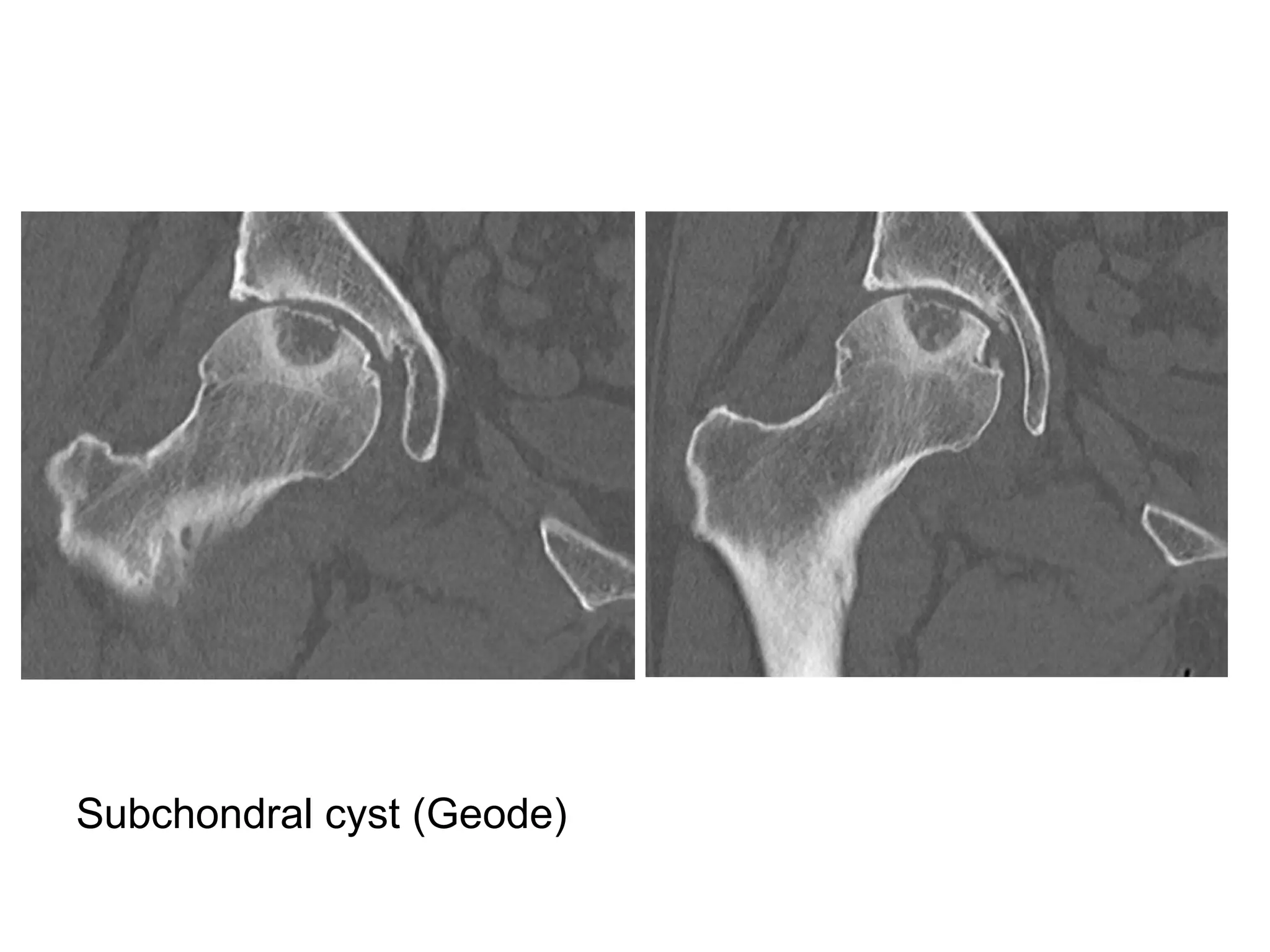


















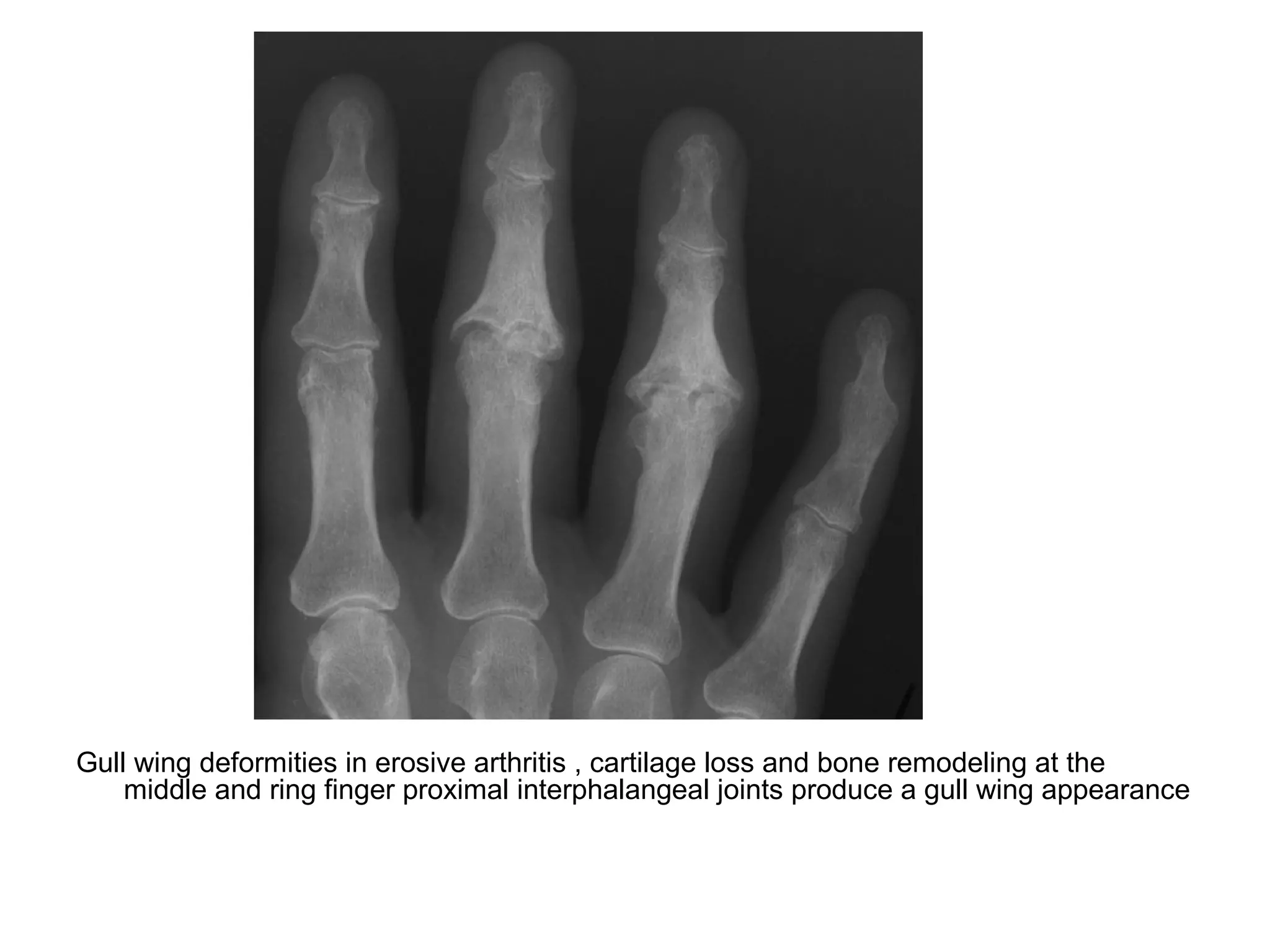








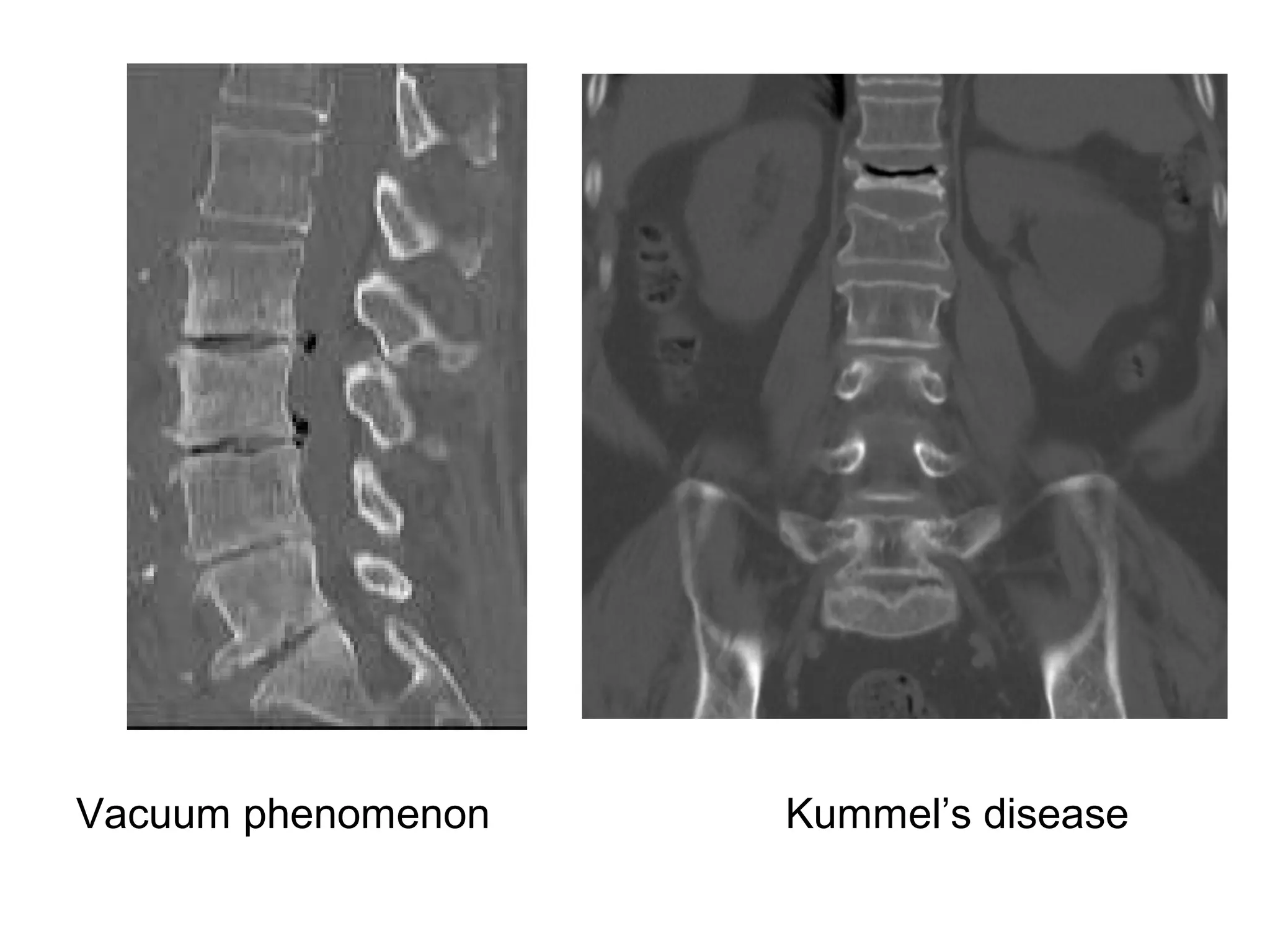
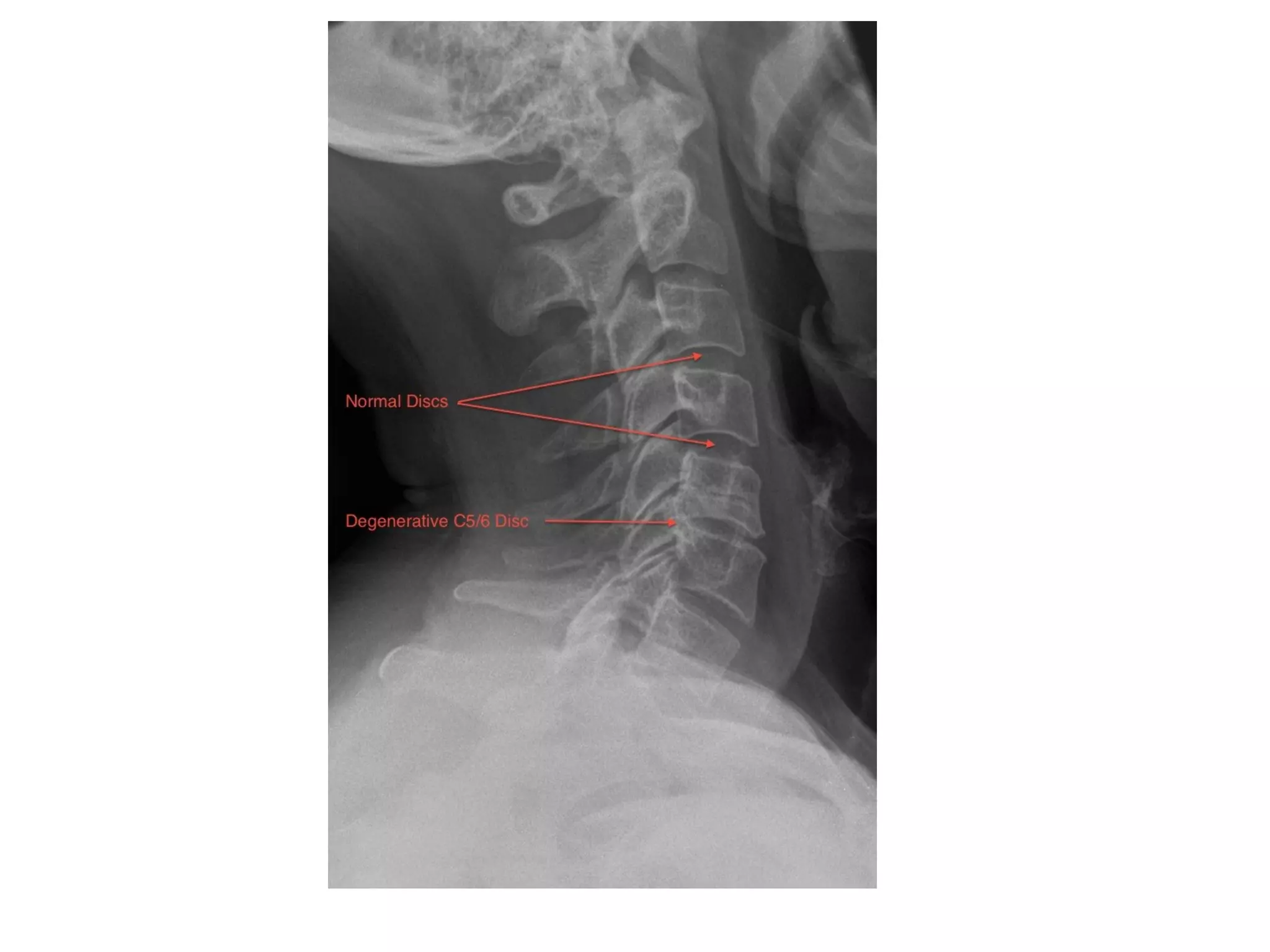
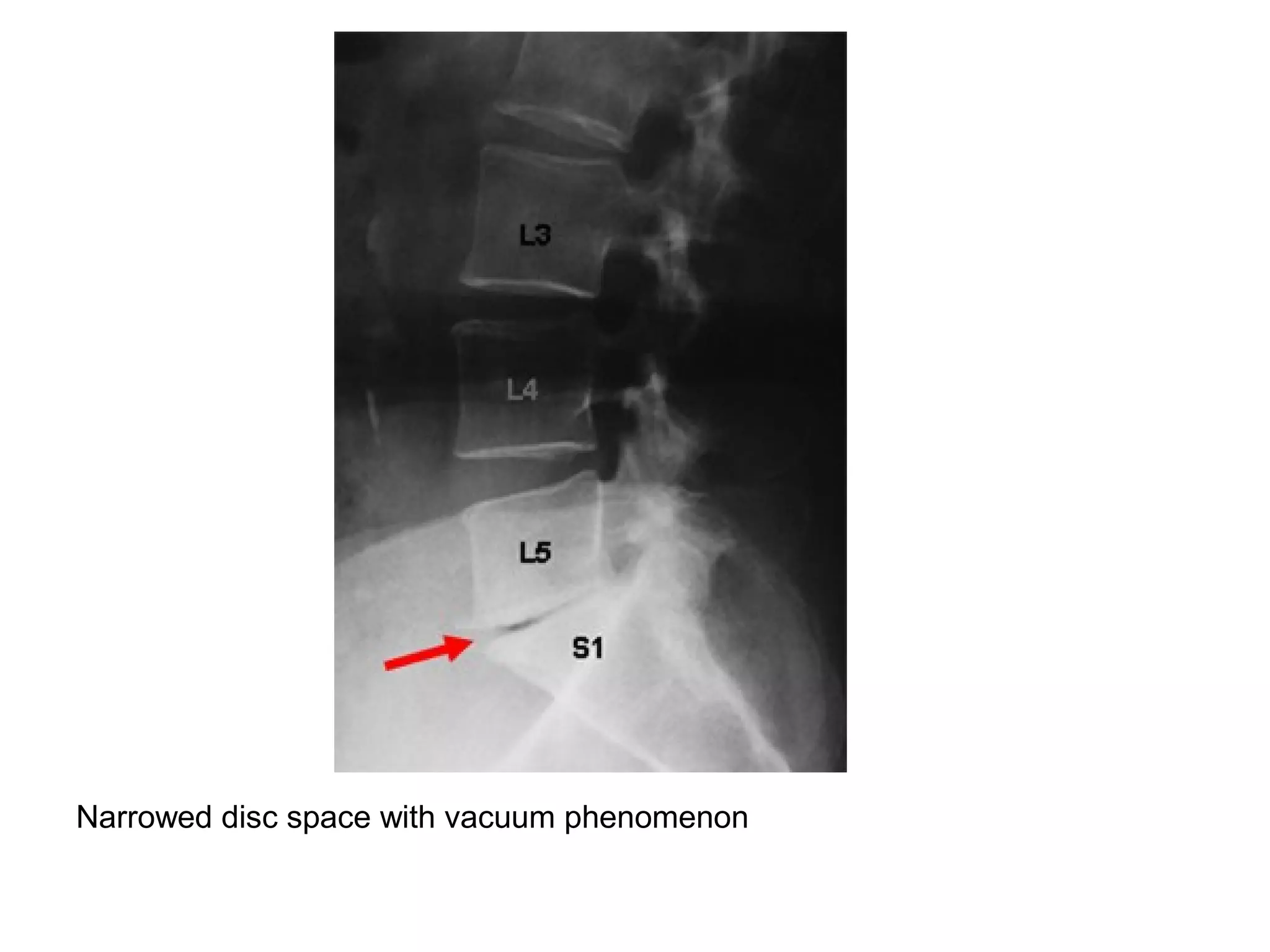








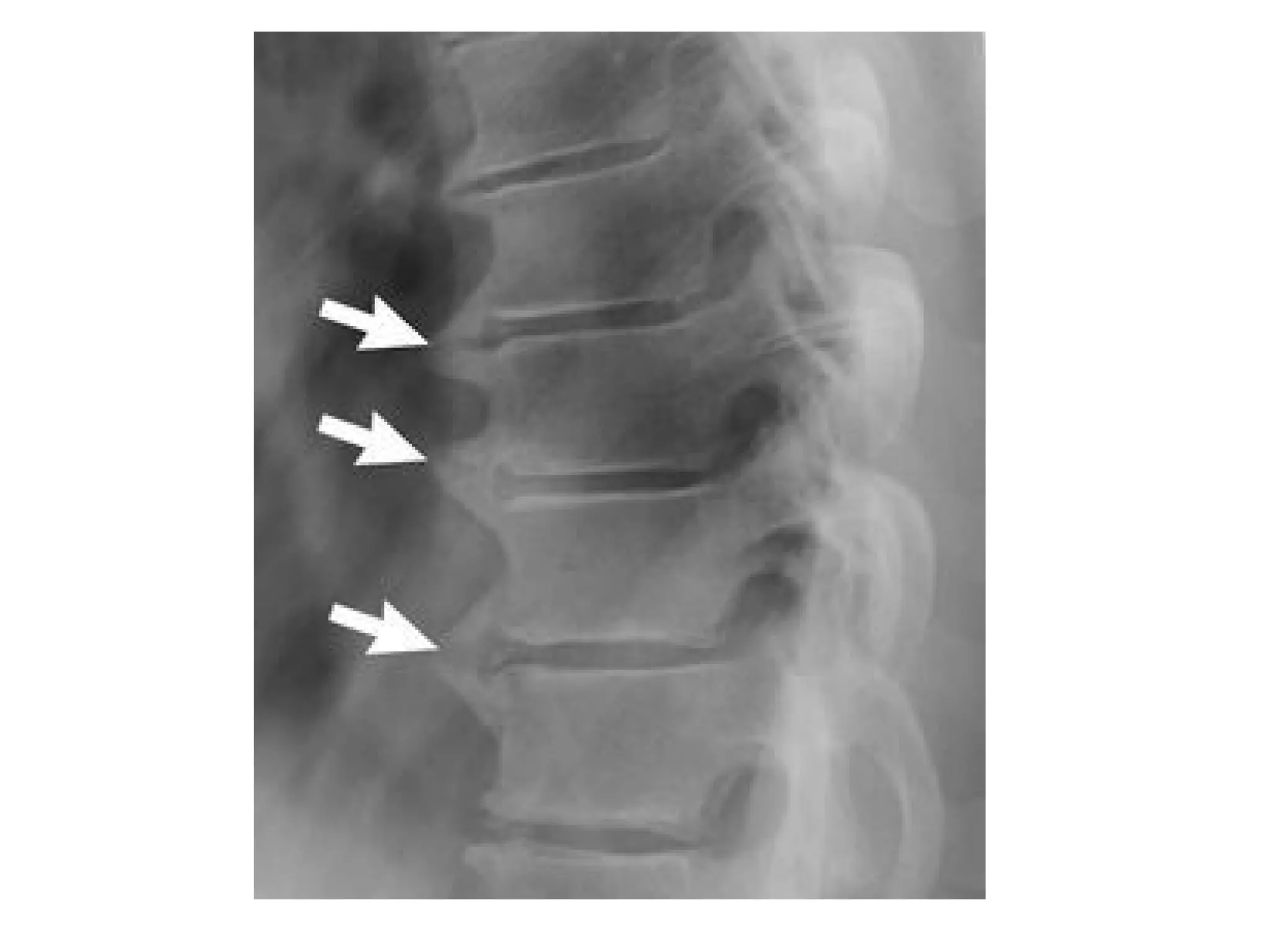







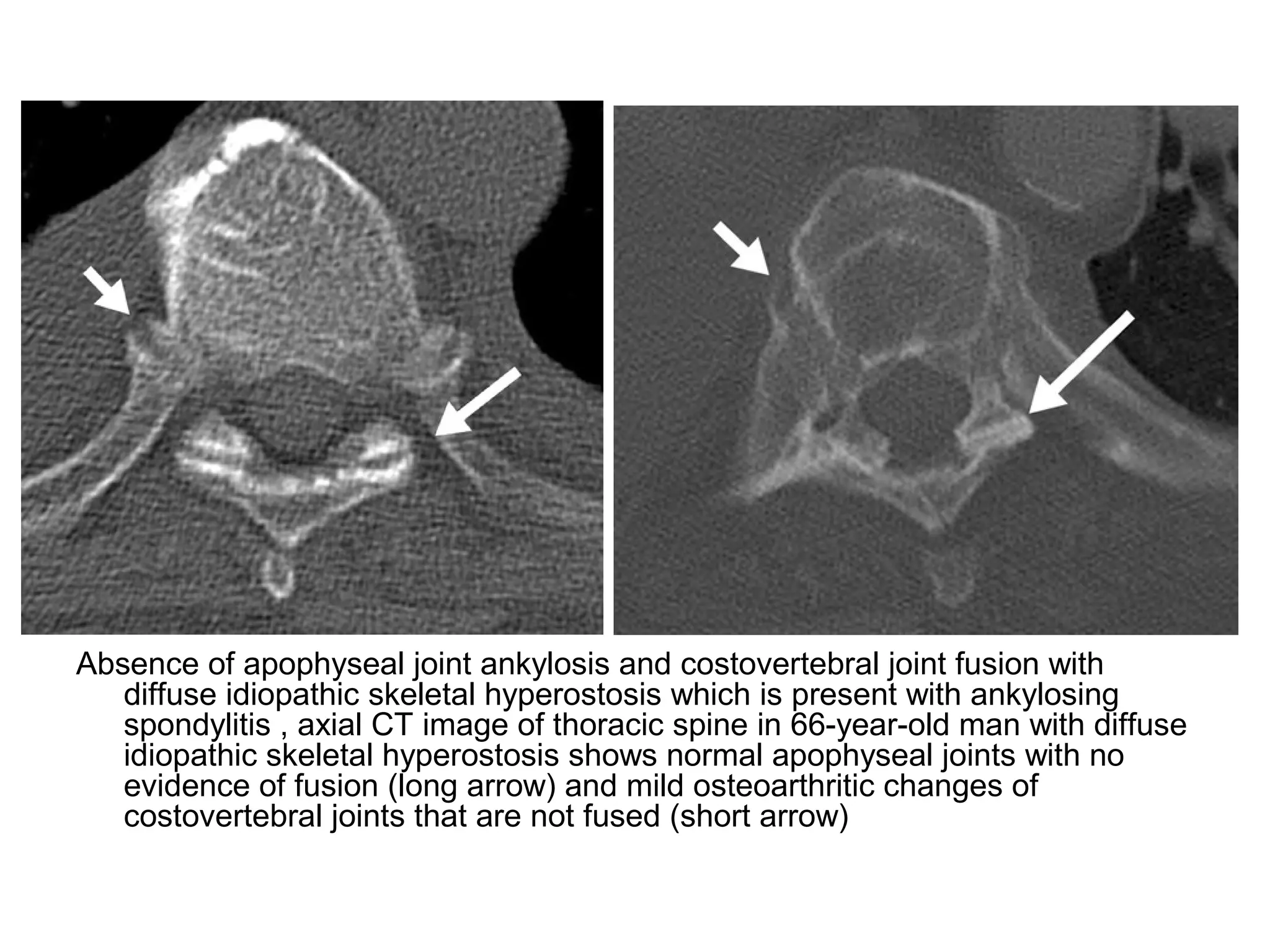





































































































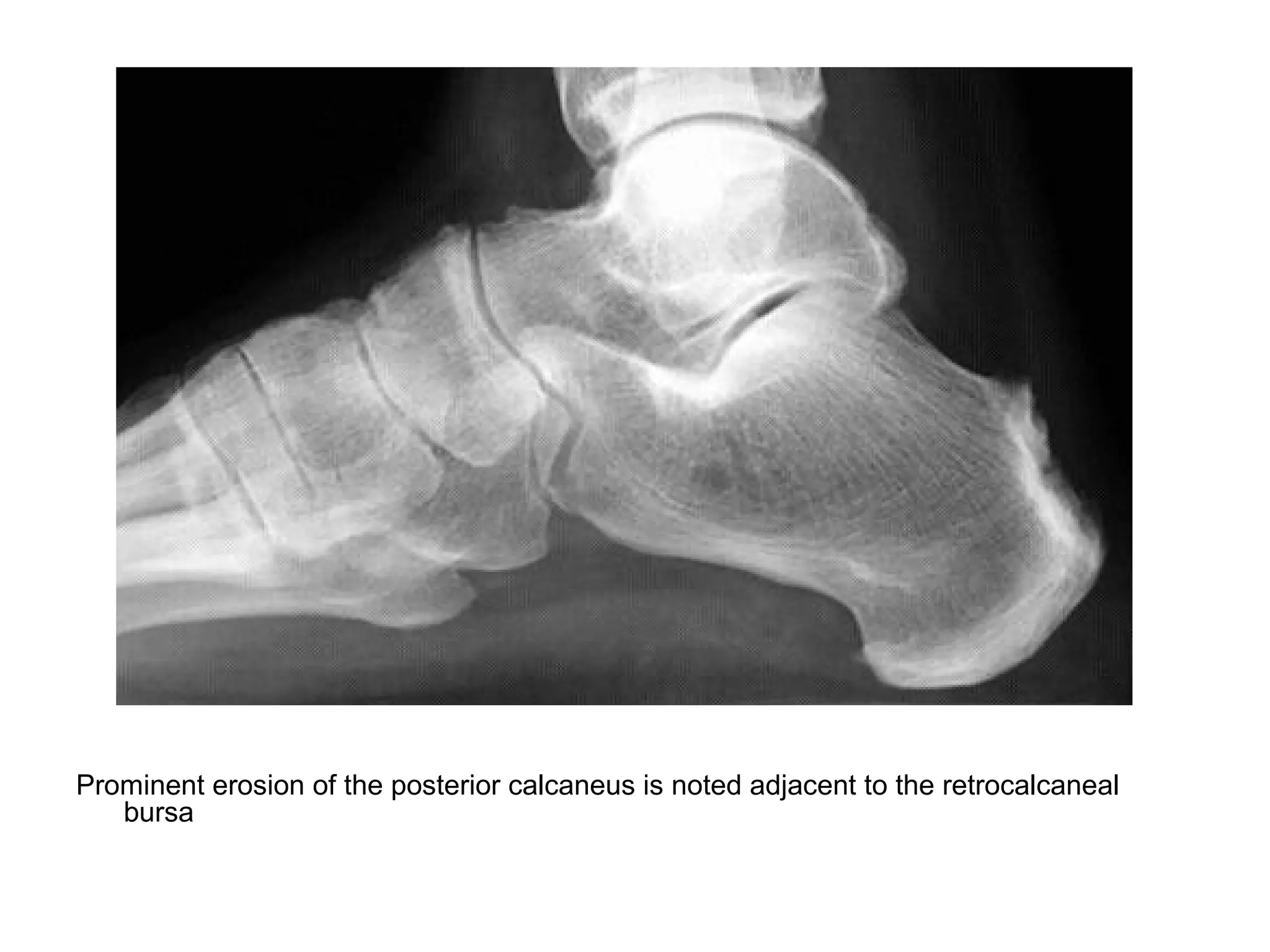
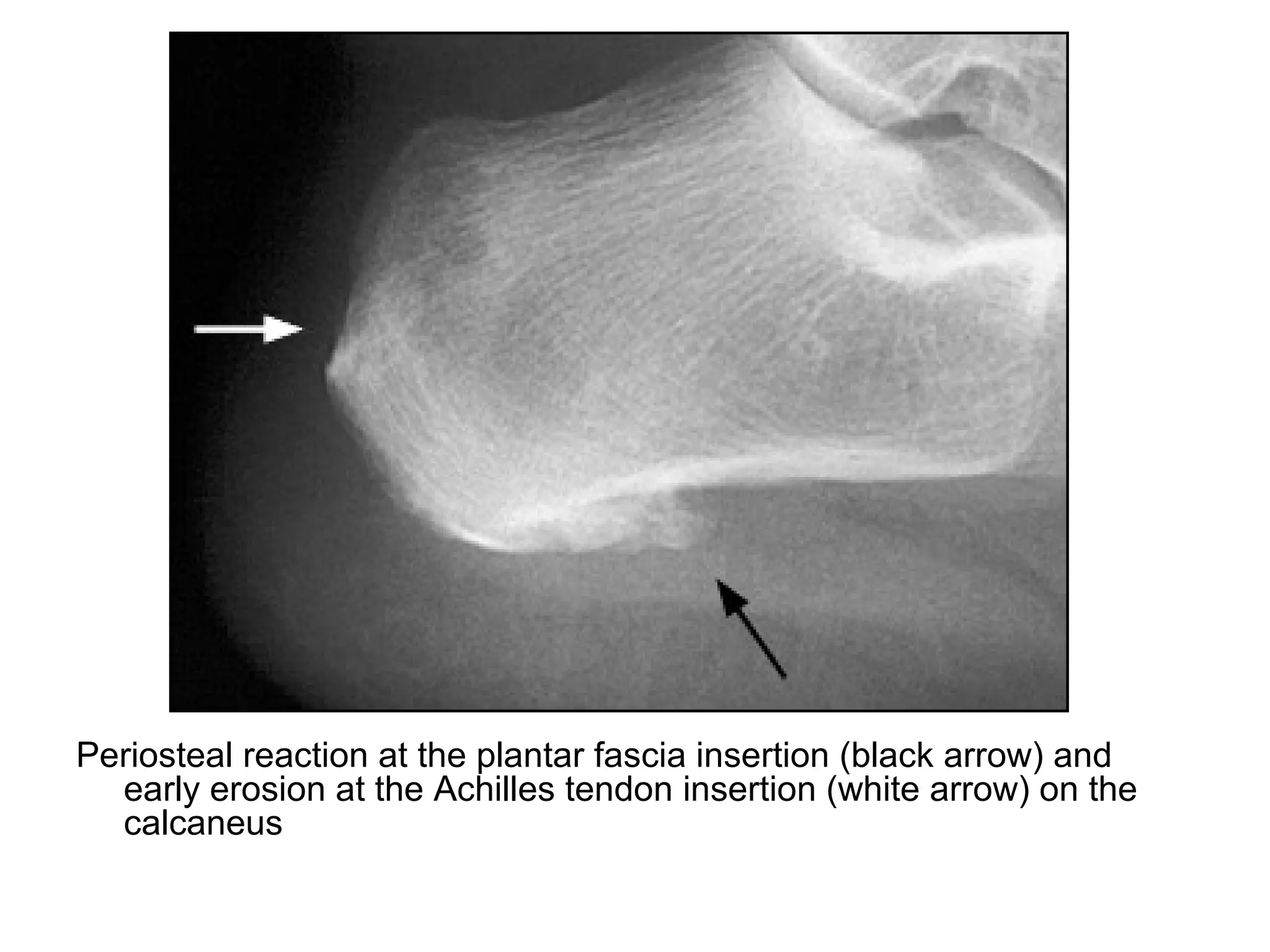
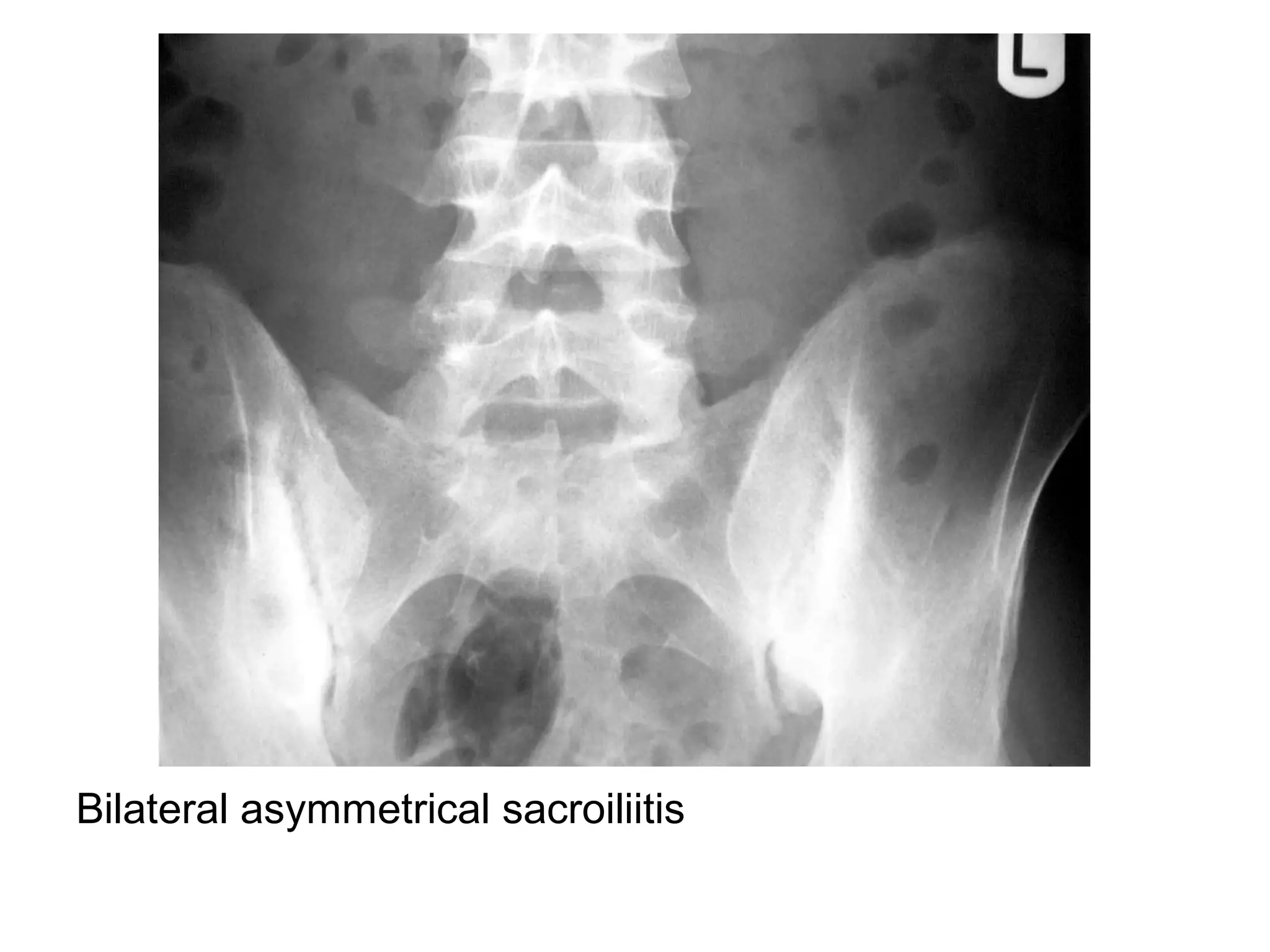























































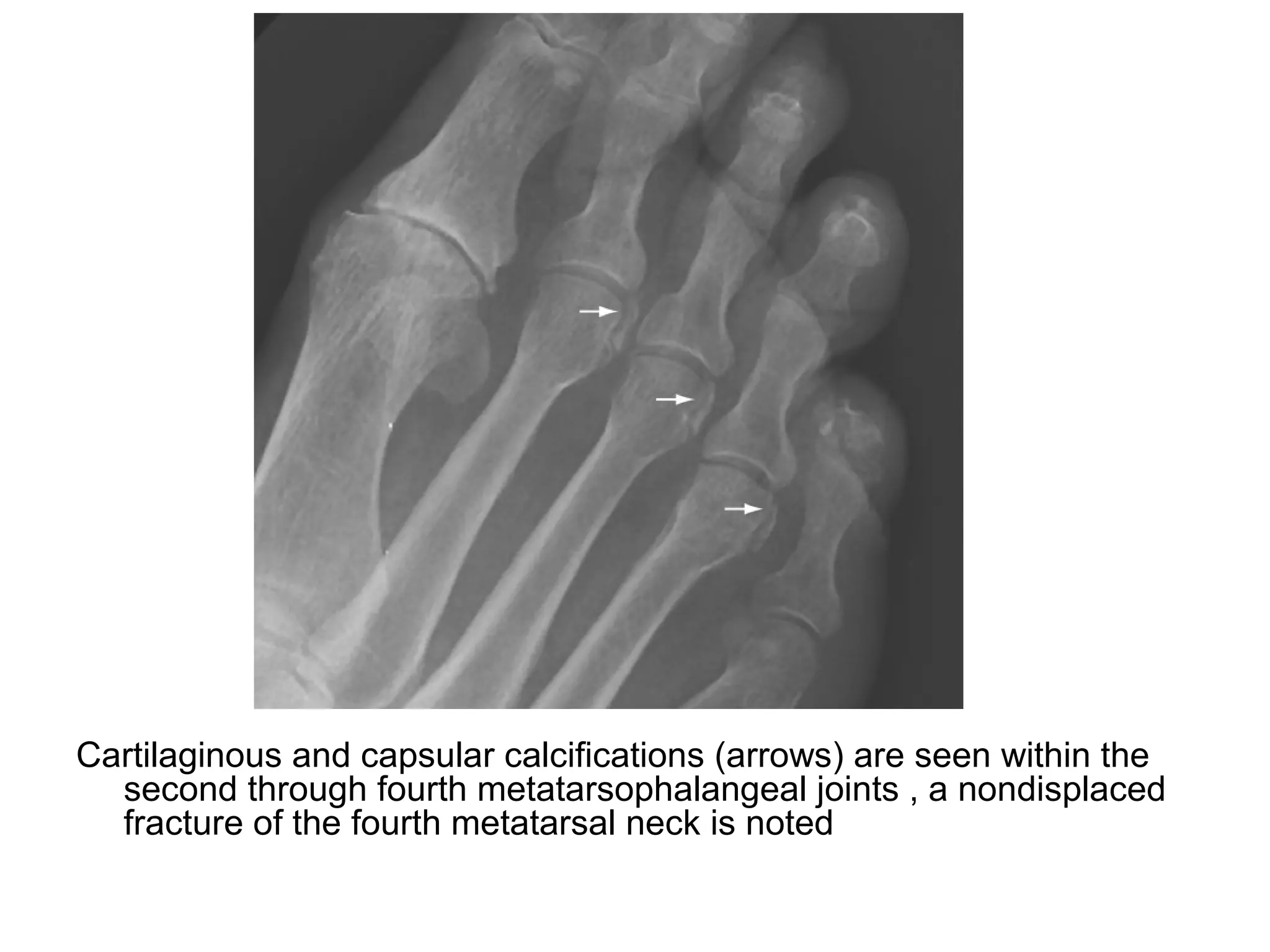



















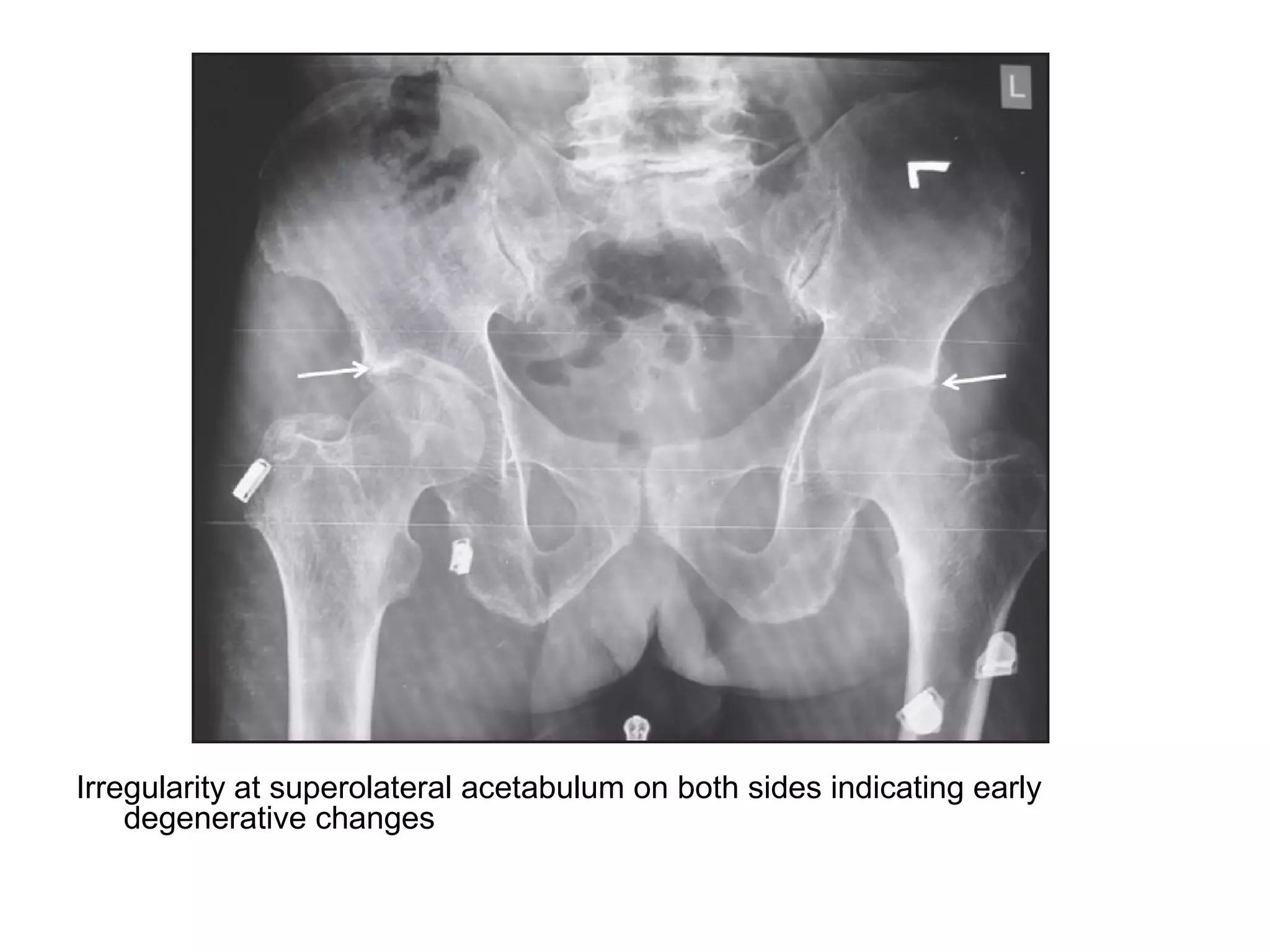



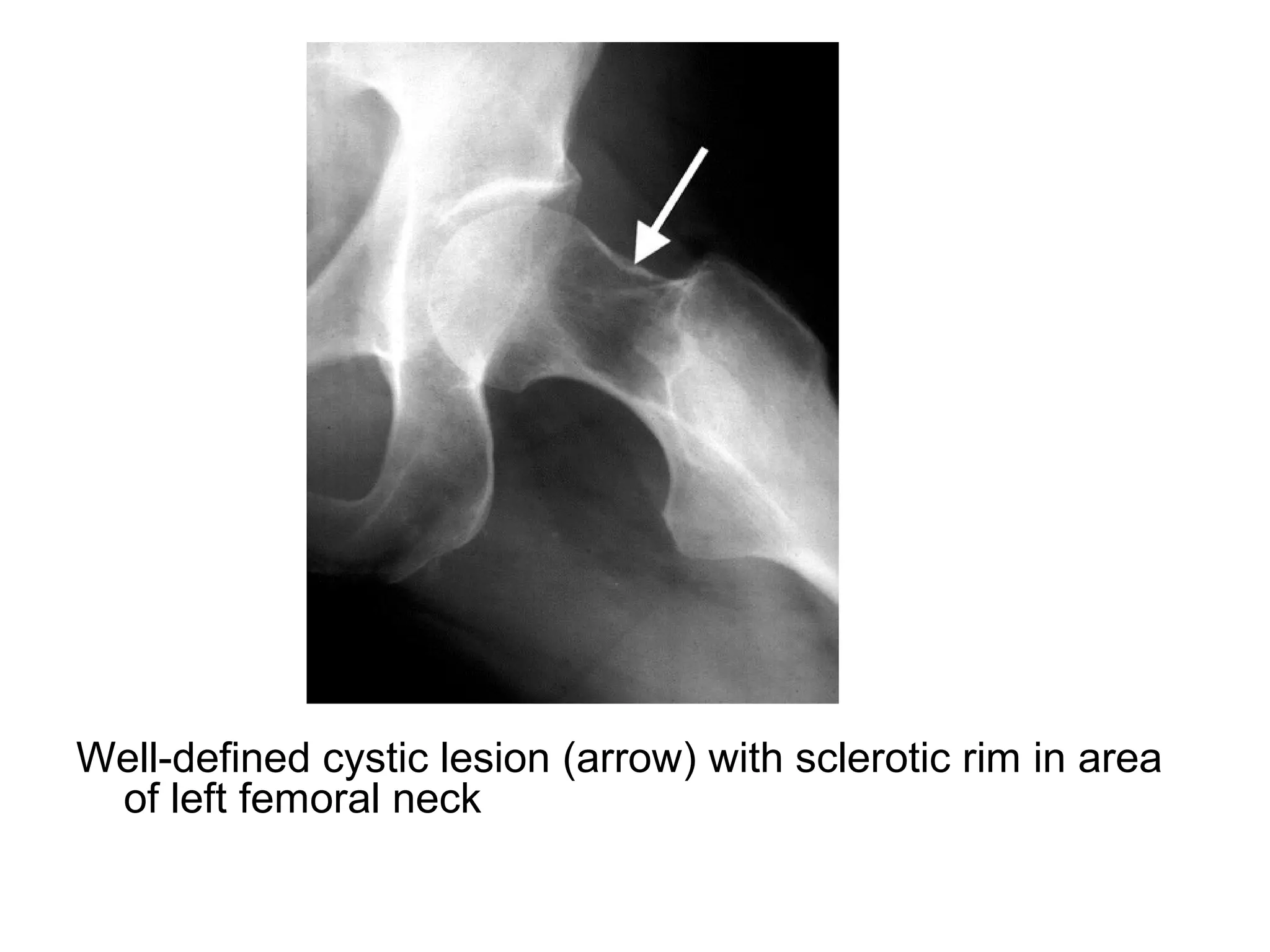

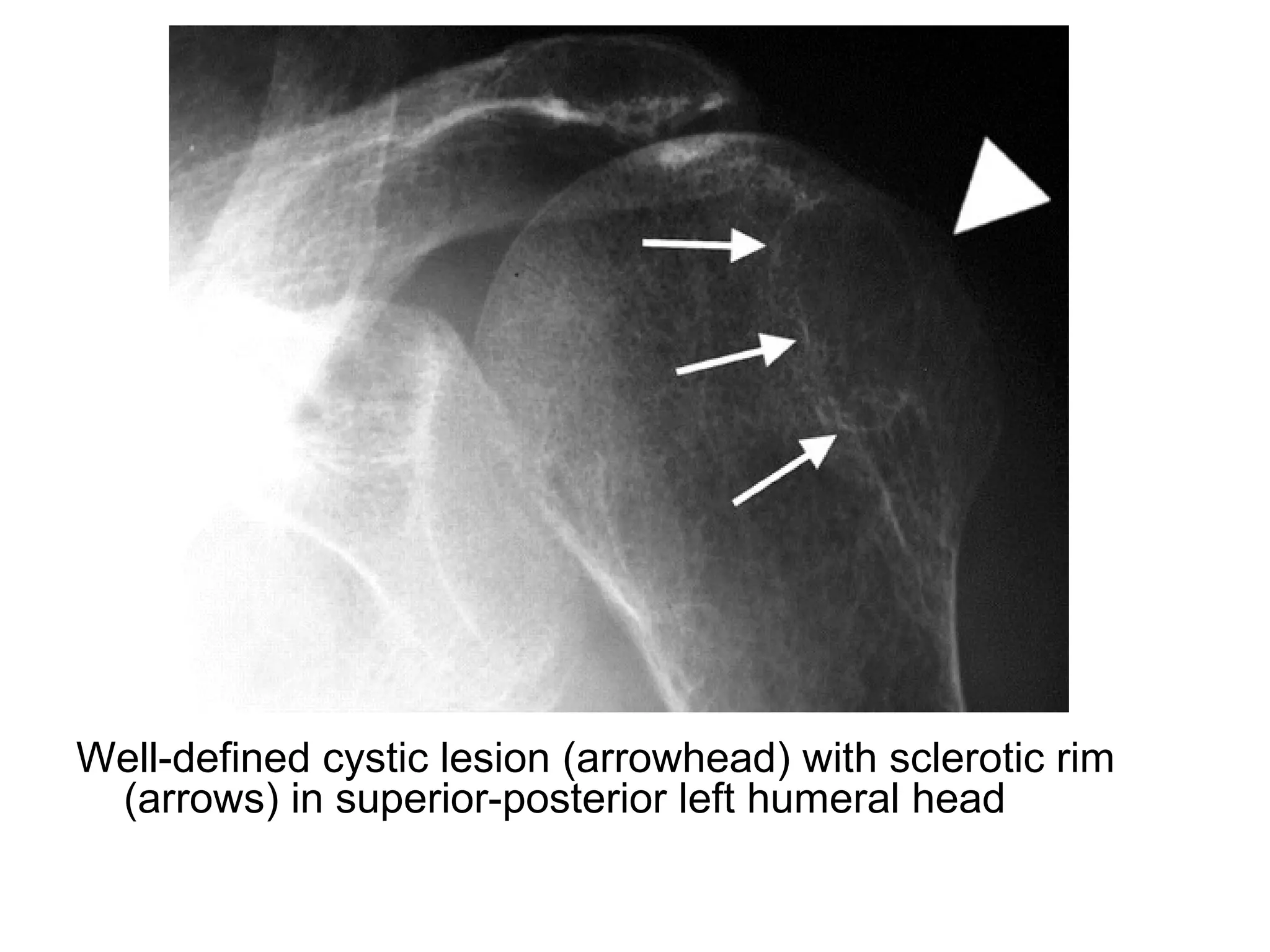














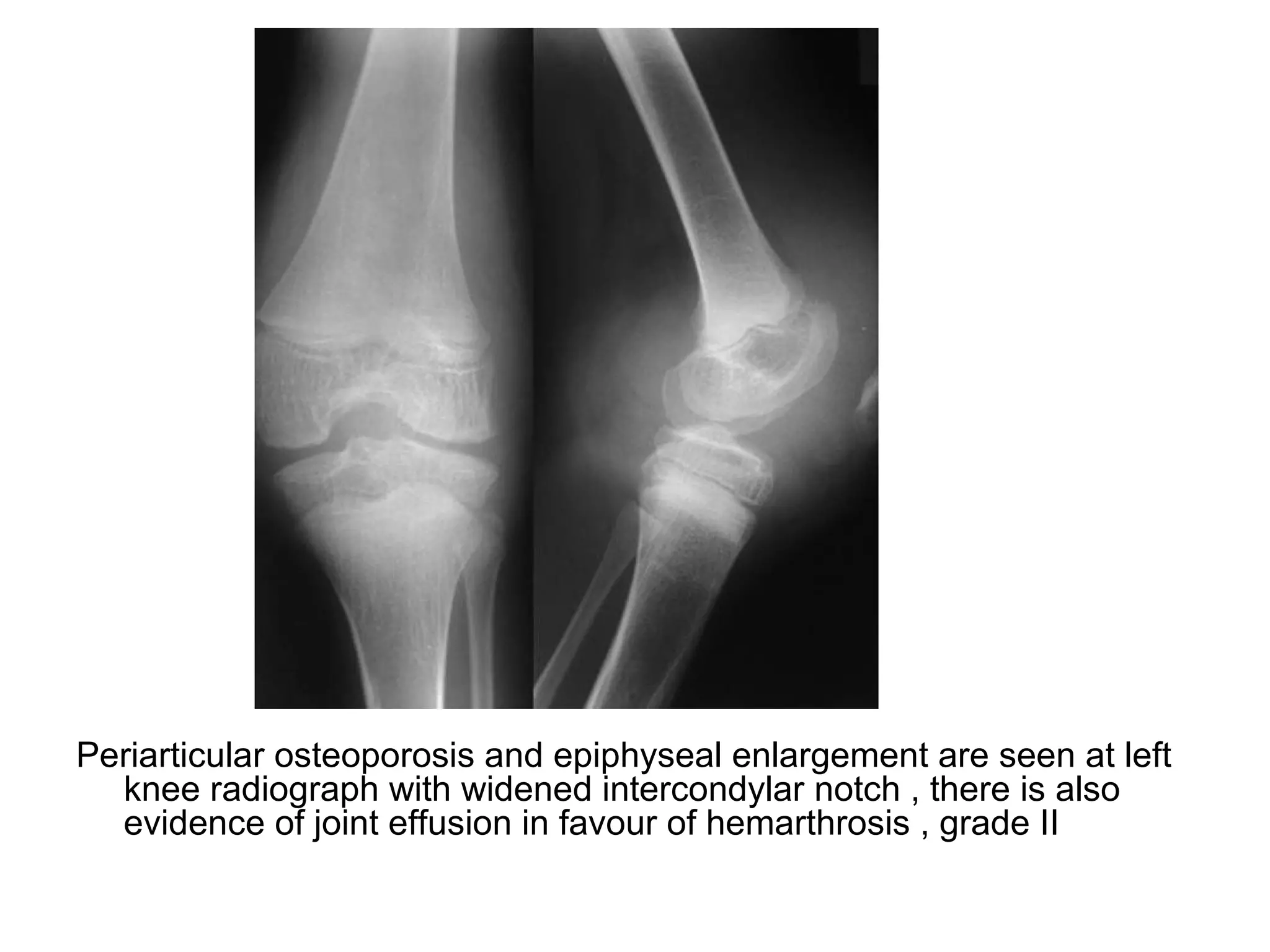


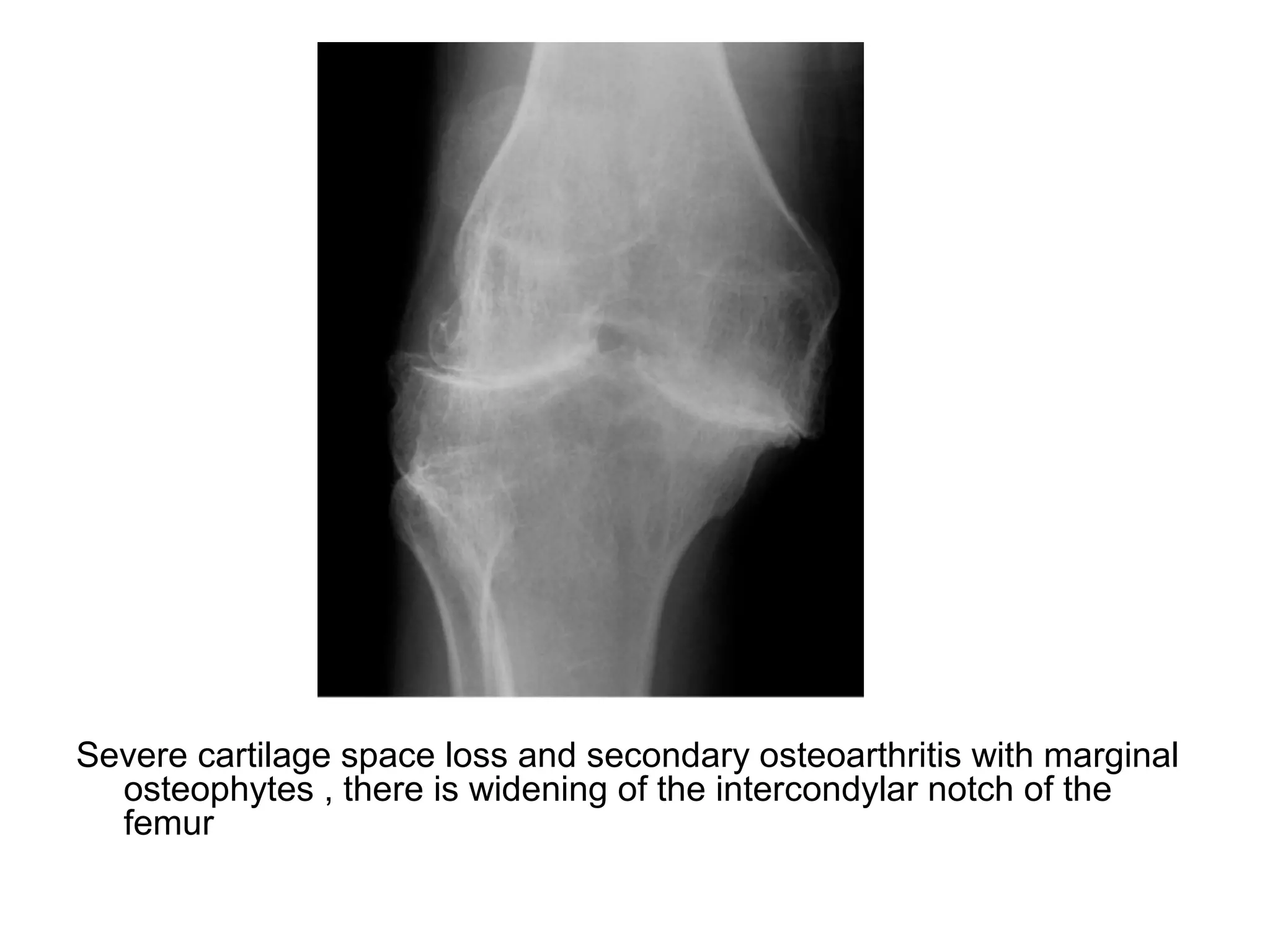

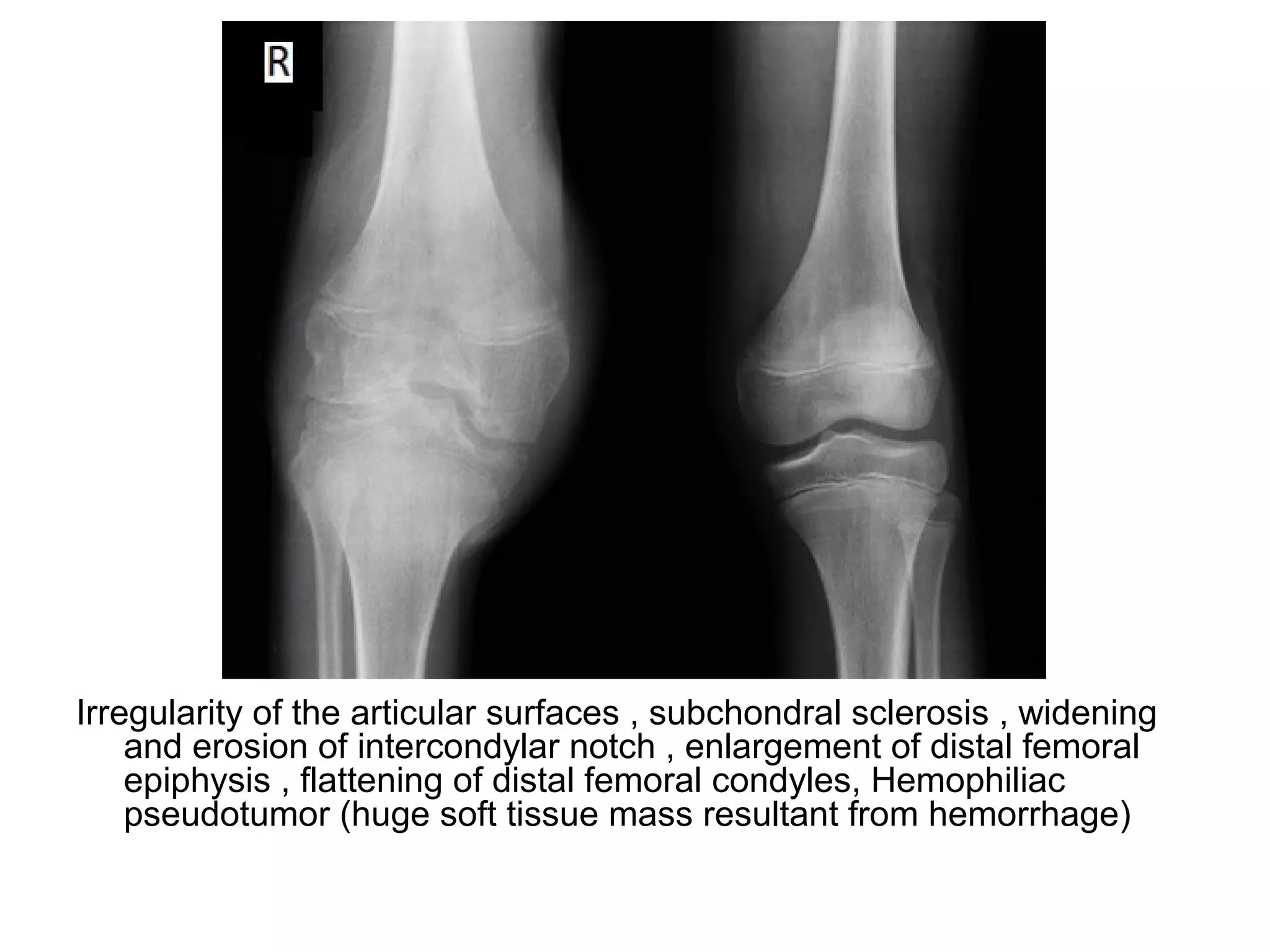

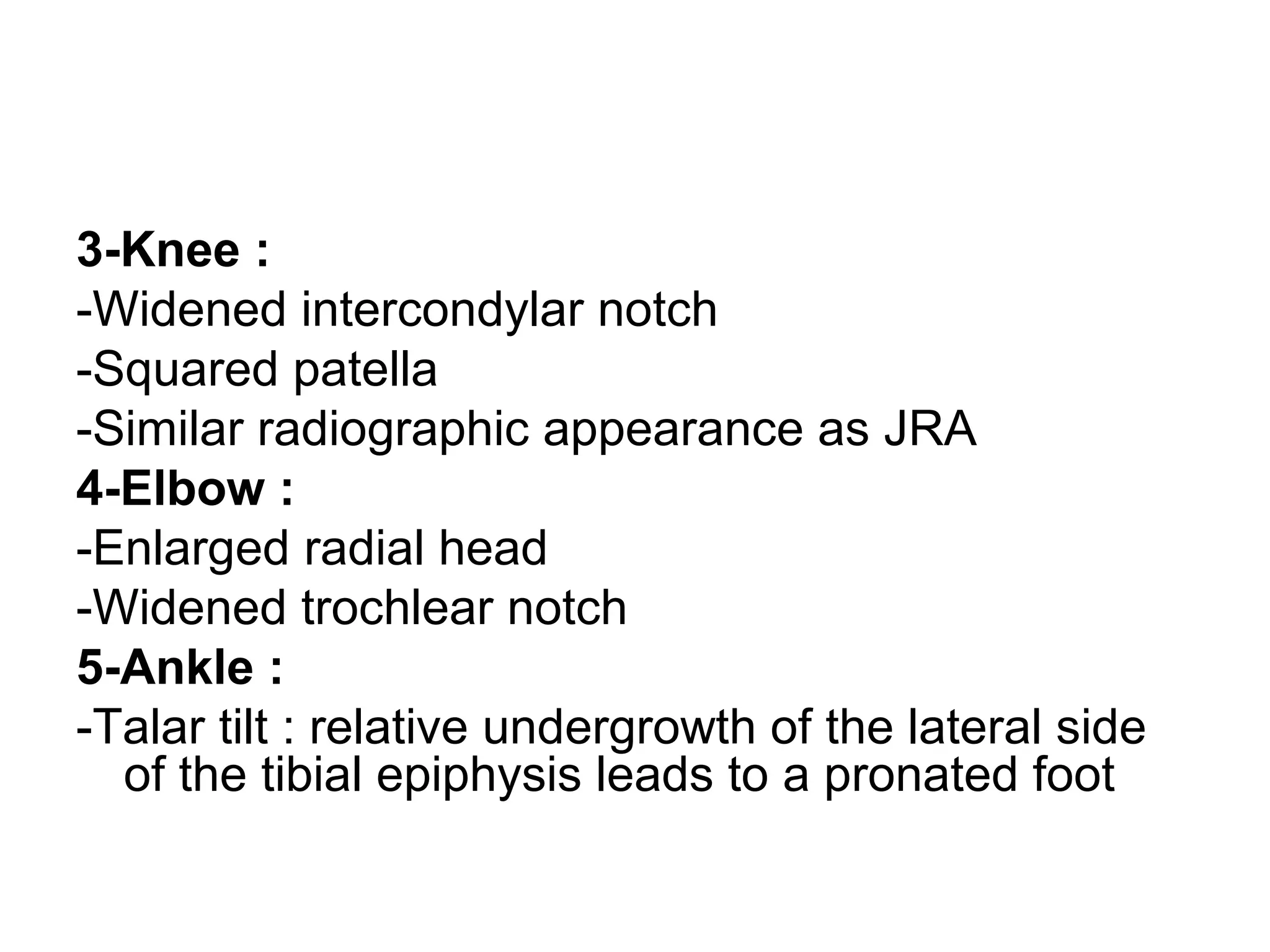





















This document provides an overview of musculoskeletal arthritis, focusing on degenerative arthritis (osteoarthritis). It discusses the general features of arthritis, then covers osteoarthritis in more detail including types, radiographic features, incidence in different joints, and related conditions like erosive osteoarthritis, degenerative disc disease, spondylosis deformans, and diffuse idiopathic skeletal hyperostosis. Radiographic images are provided to illustrate findings.



























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)















