Download as PDF, PPTX
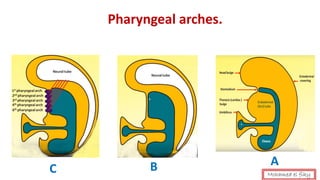

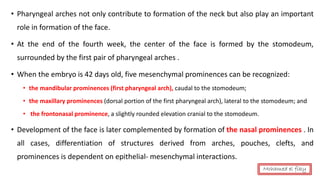
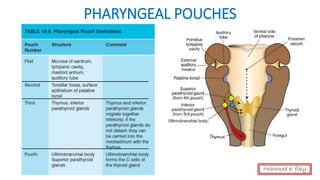
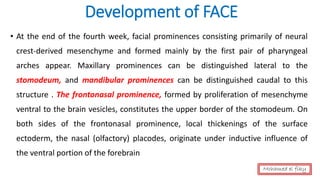
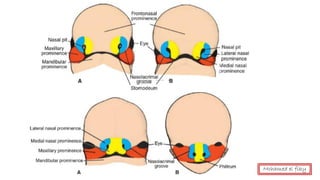

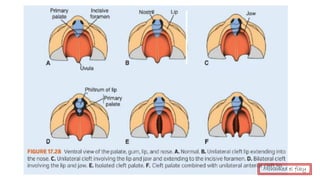
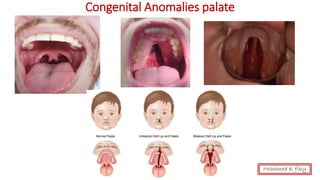
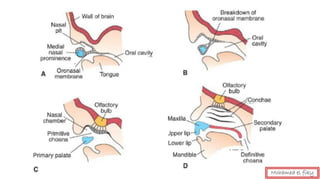

The document discusses the development of structures in the head and neck region from pharyngeal arches and pouches during weeks 4-8 of human embryo development. Key structures that develop include: - Pharyngeal arches contribute to formation of face, tongue, palate, and nasal cavity. Pharyngeal pouches form parts of throat and ear. - Tongue develops from swellings in the first pharyngeal arch. Palate develops from the intermaxillary segment and palatine shelves fusing. Nose develops from five facial prominences. - Structures of the face, neck, and throat are innervated by cranial nerves associated with their pharyngeal arch of origin. Abnormal























































![Anatomy of Male genital organs [auto saved]](https://cdn.slidesharecdn.com/ss_thumbnails/malegenitalorgansauto-saved-200818065025-thumbnail.jpg?width=640&height=640&fit=bounds)

![anatomy of Female genital organs [auto saved]](https://cdn.slidesharecdn.com/ss_thumbnails/femalegenitalorgansauto-saved-200818064612-thumbnail.jpg?width=640&height=640&fit=bounds)





























