Downloaded 622 times
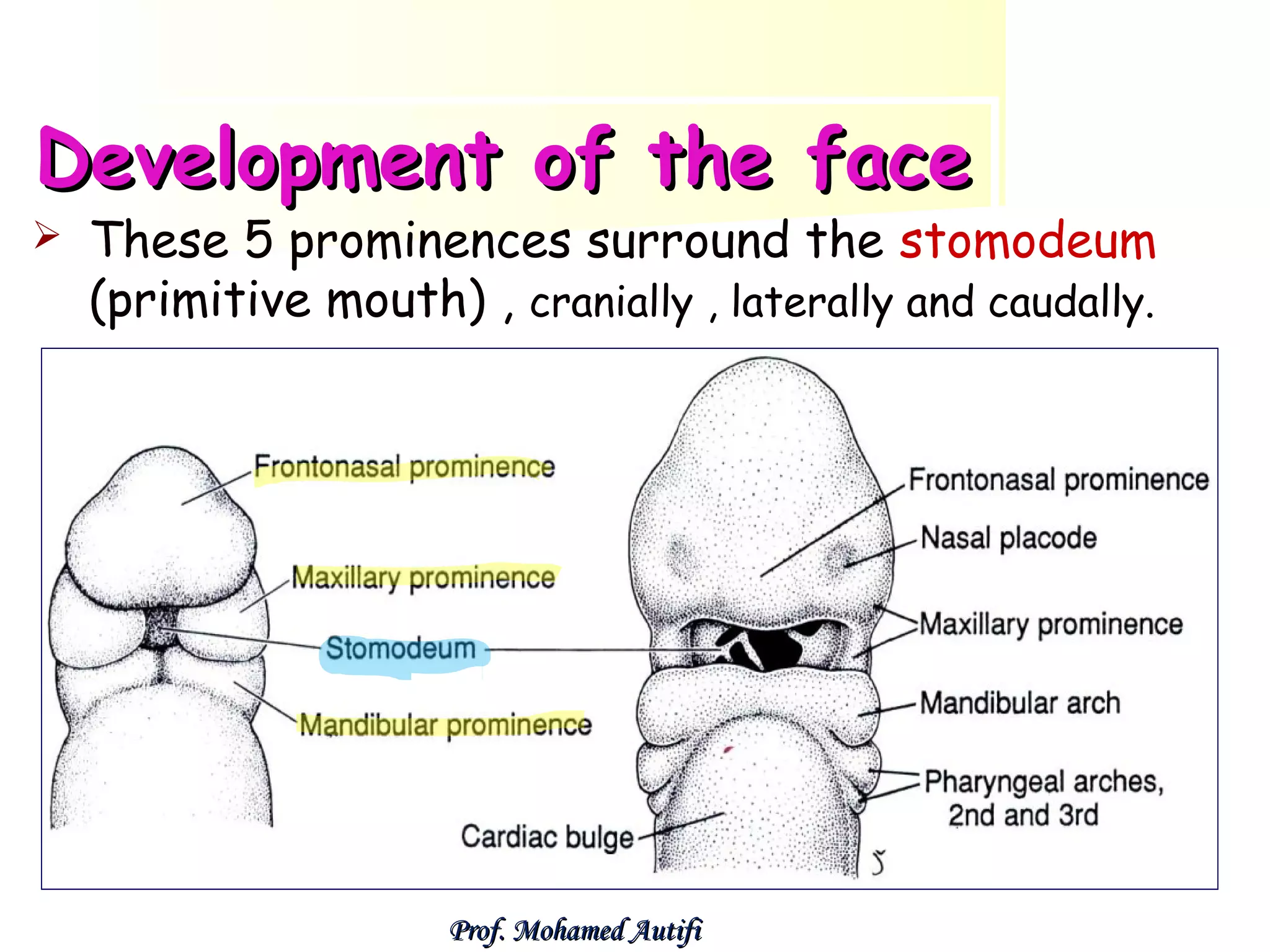
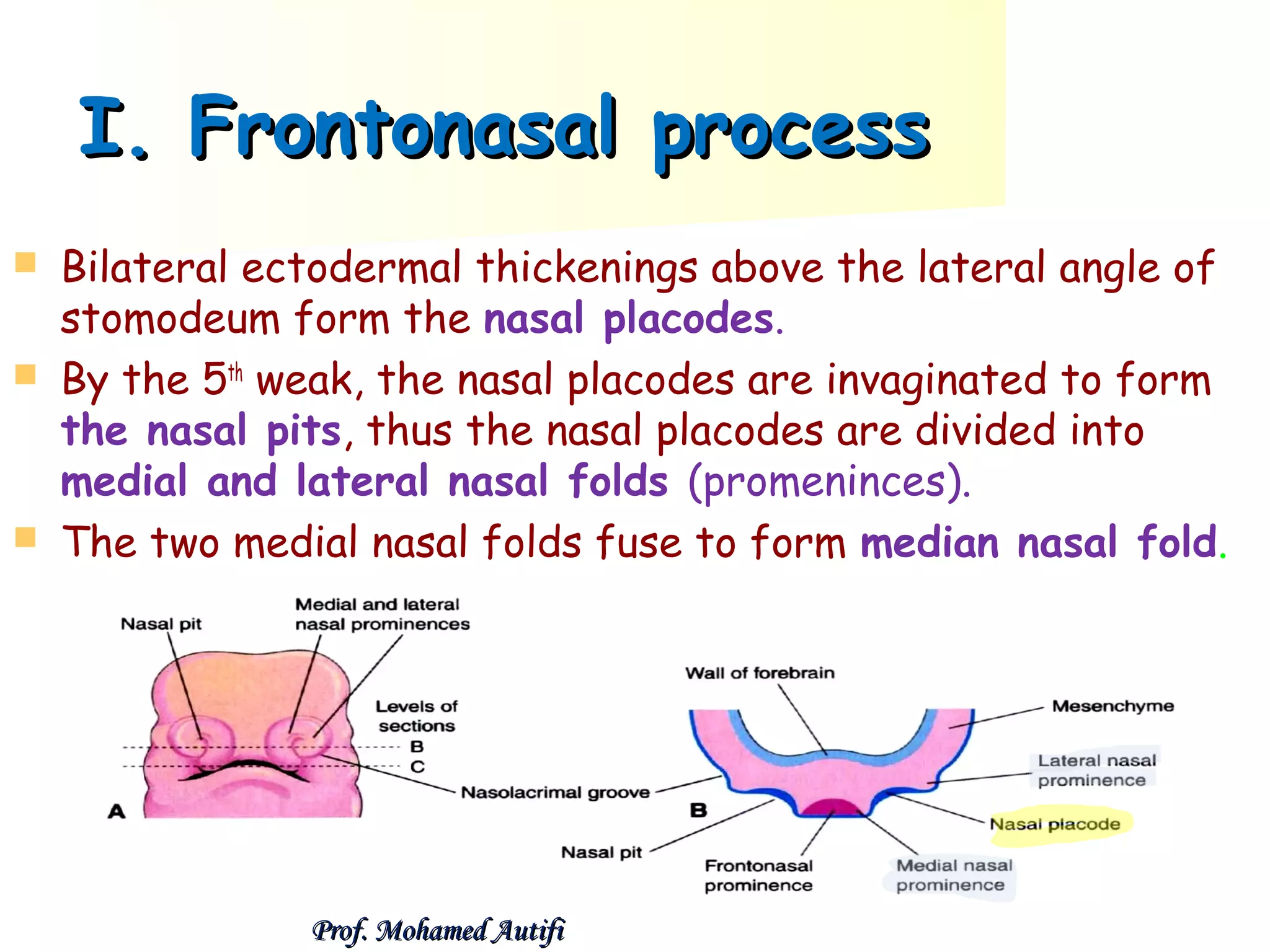
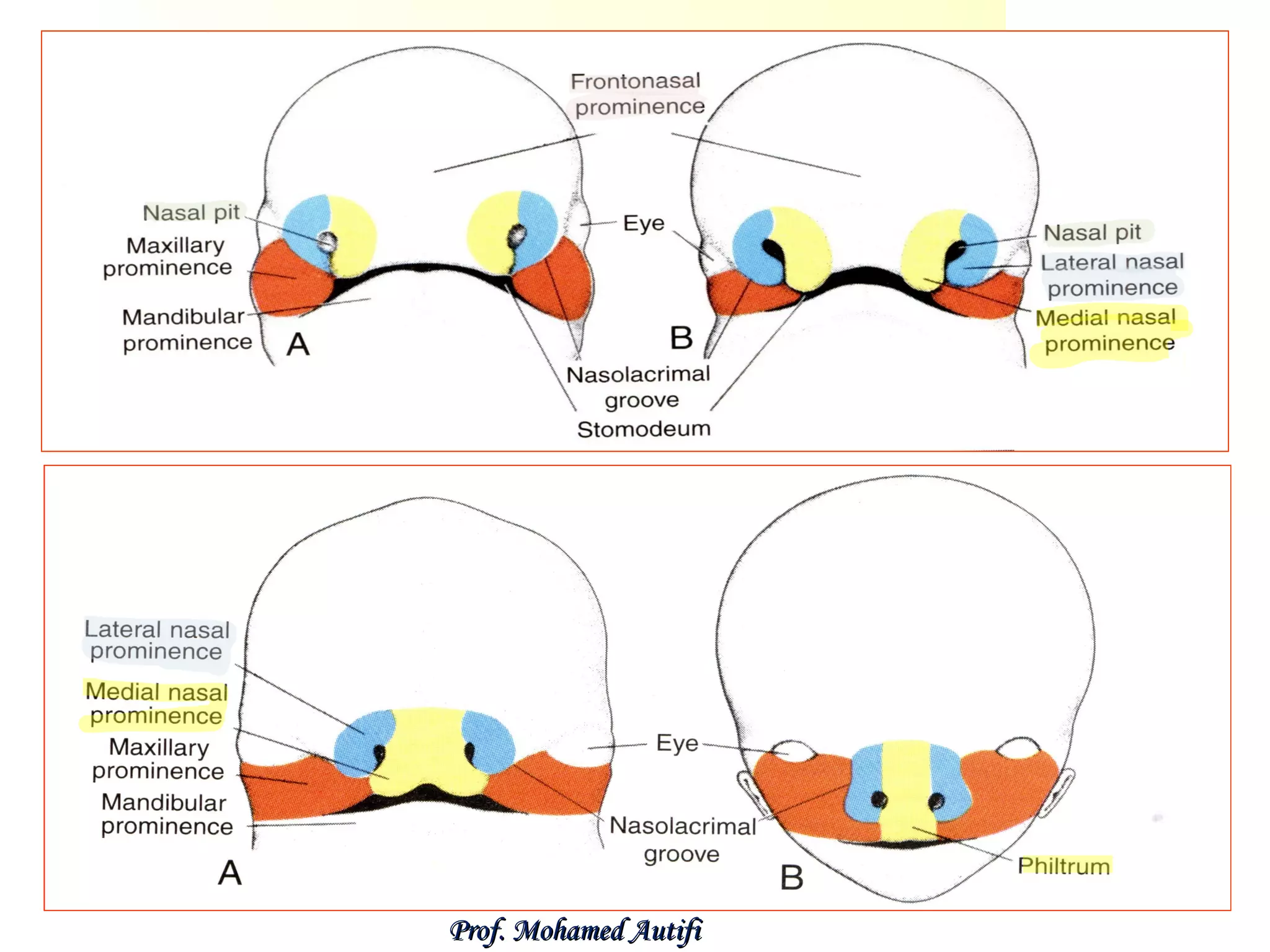
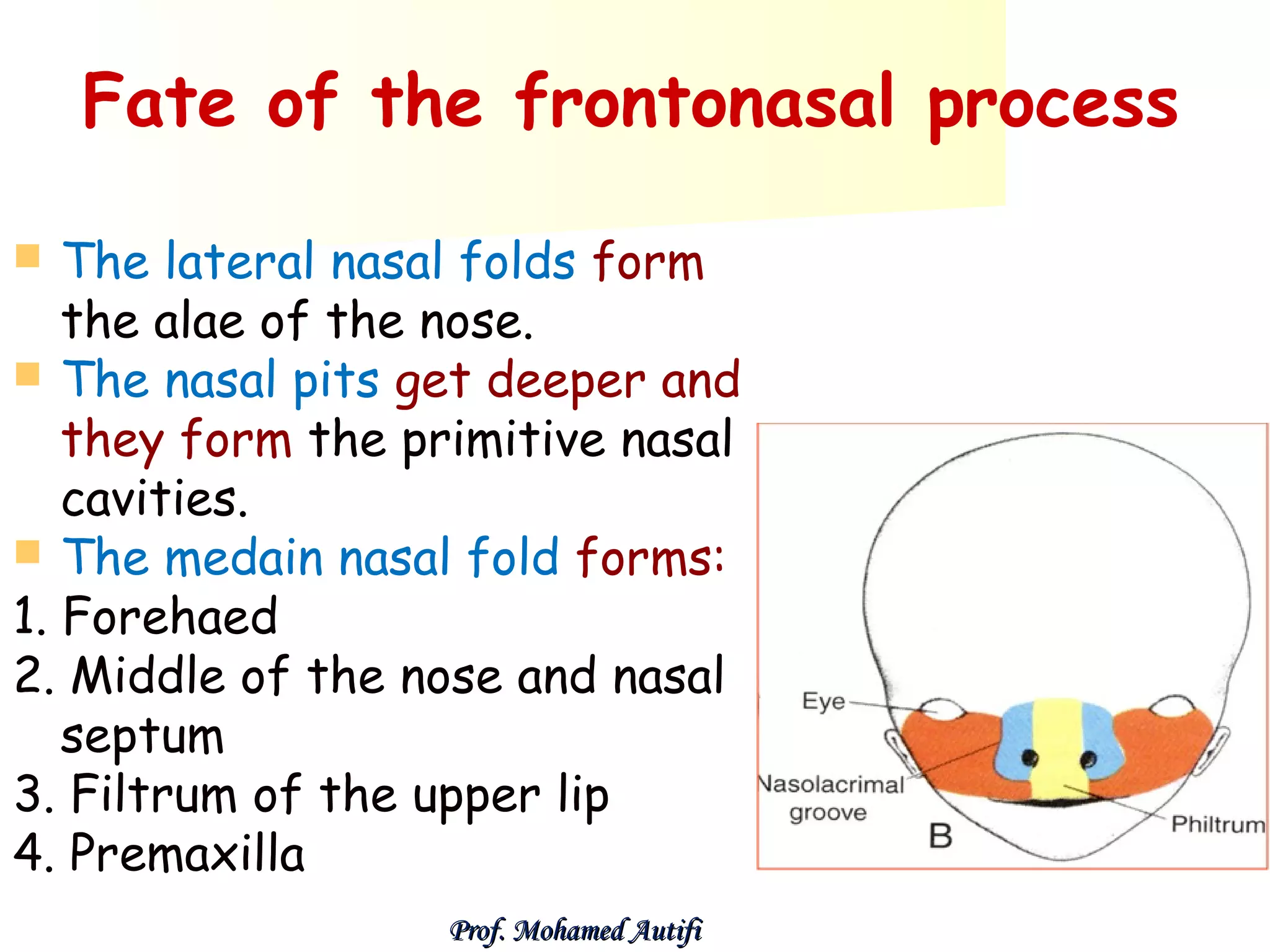
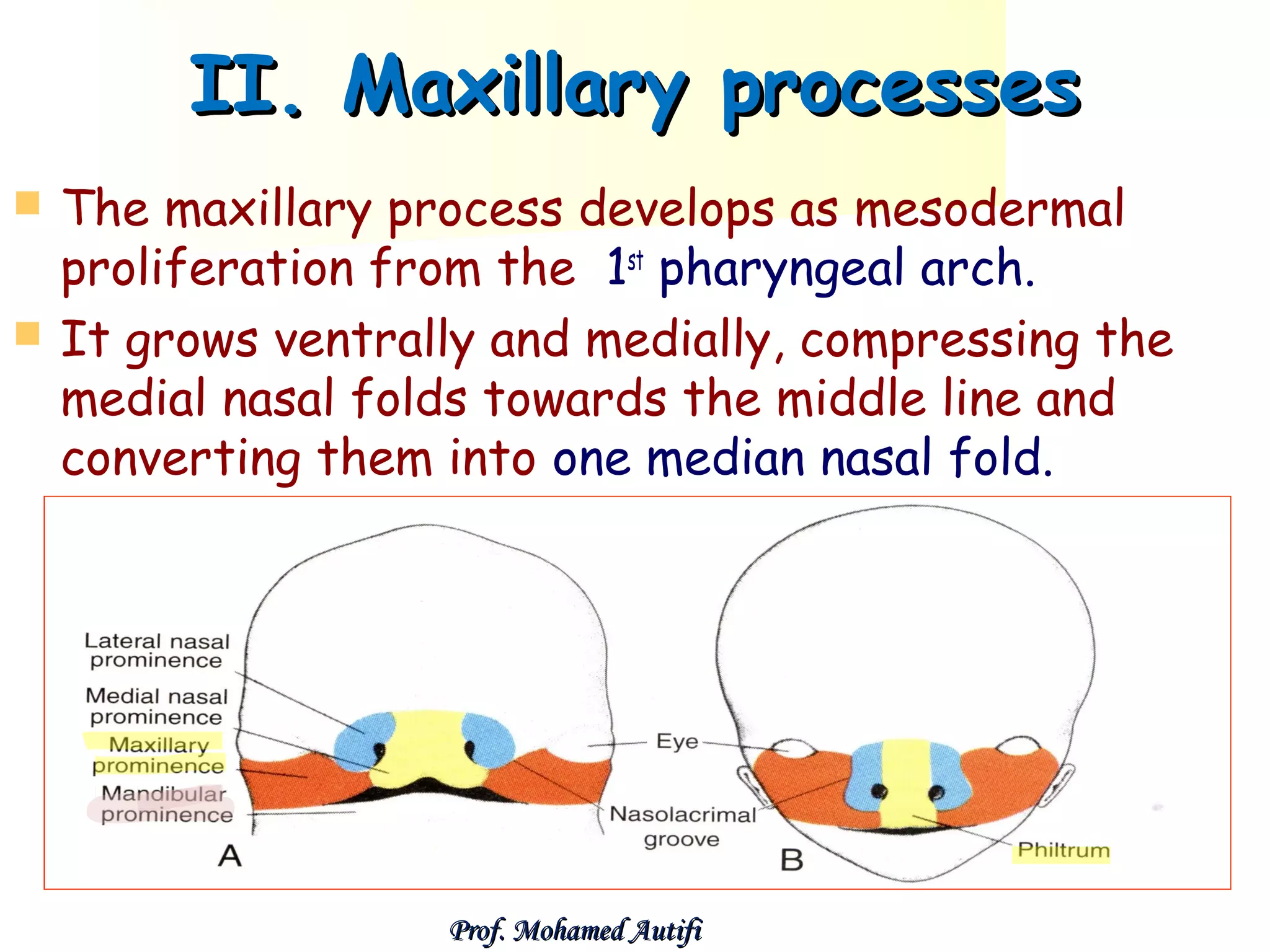
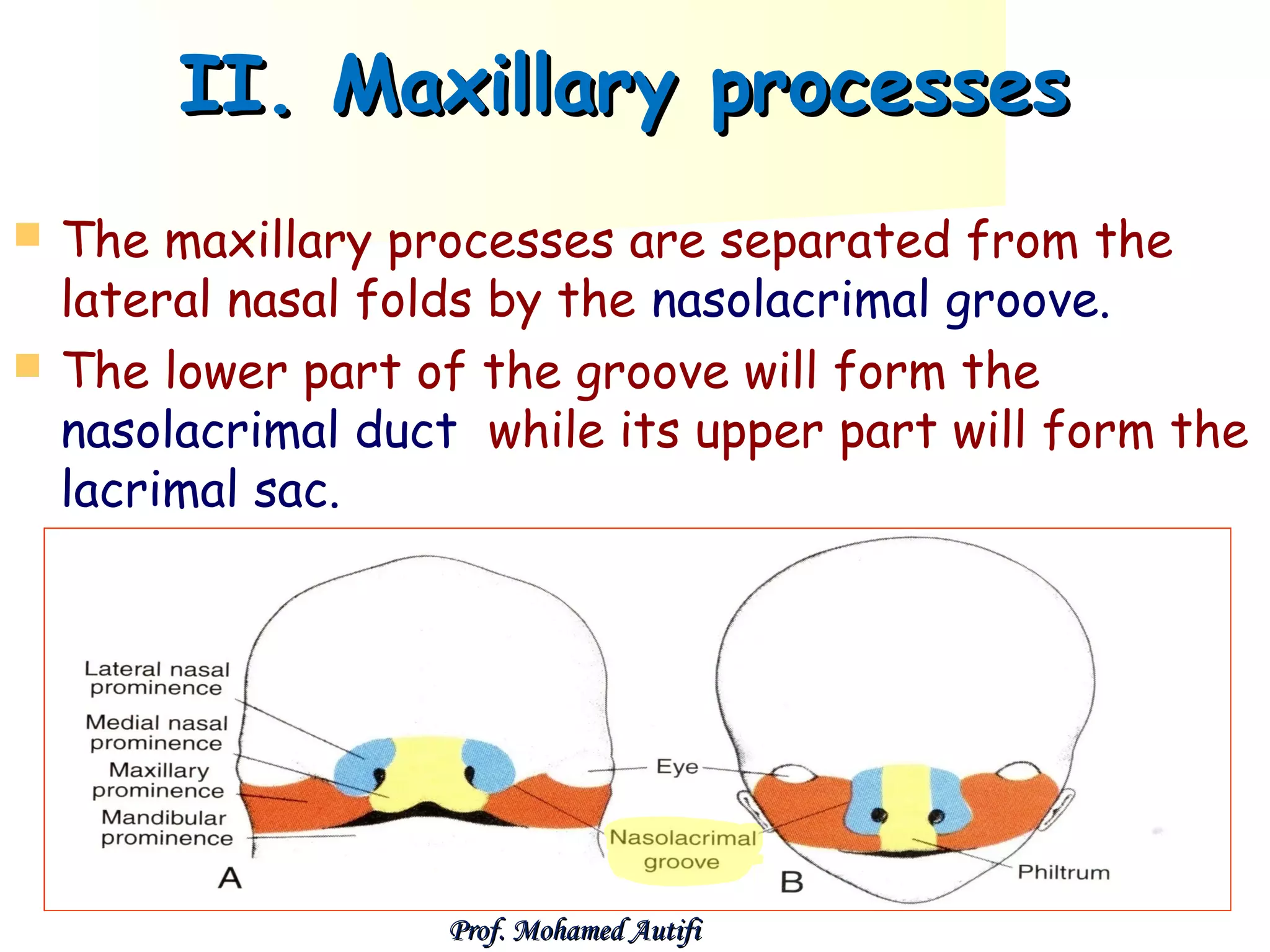
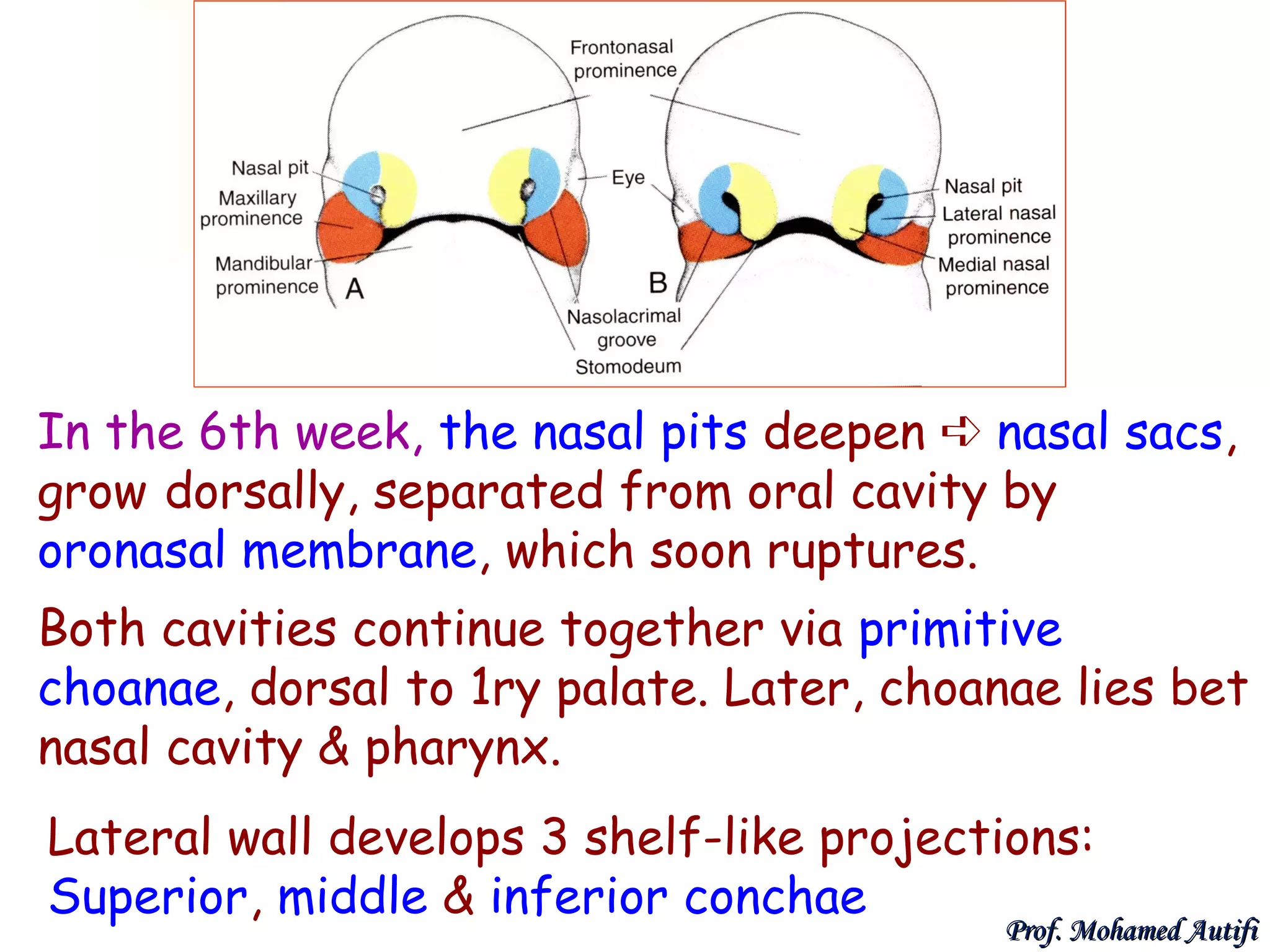
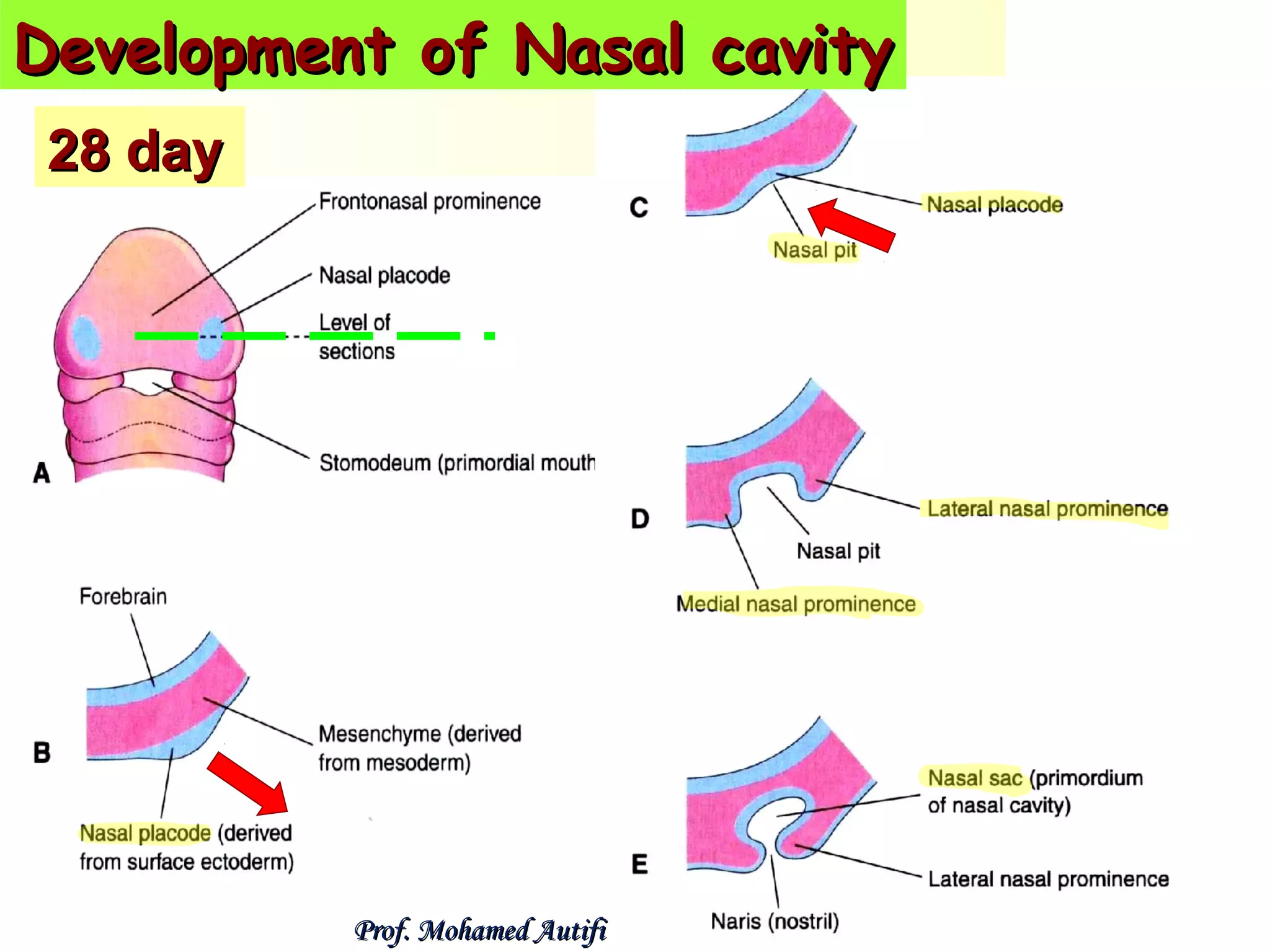
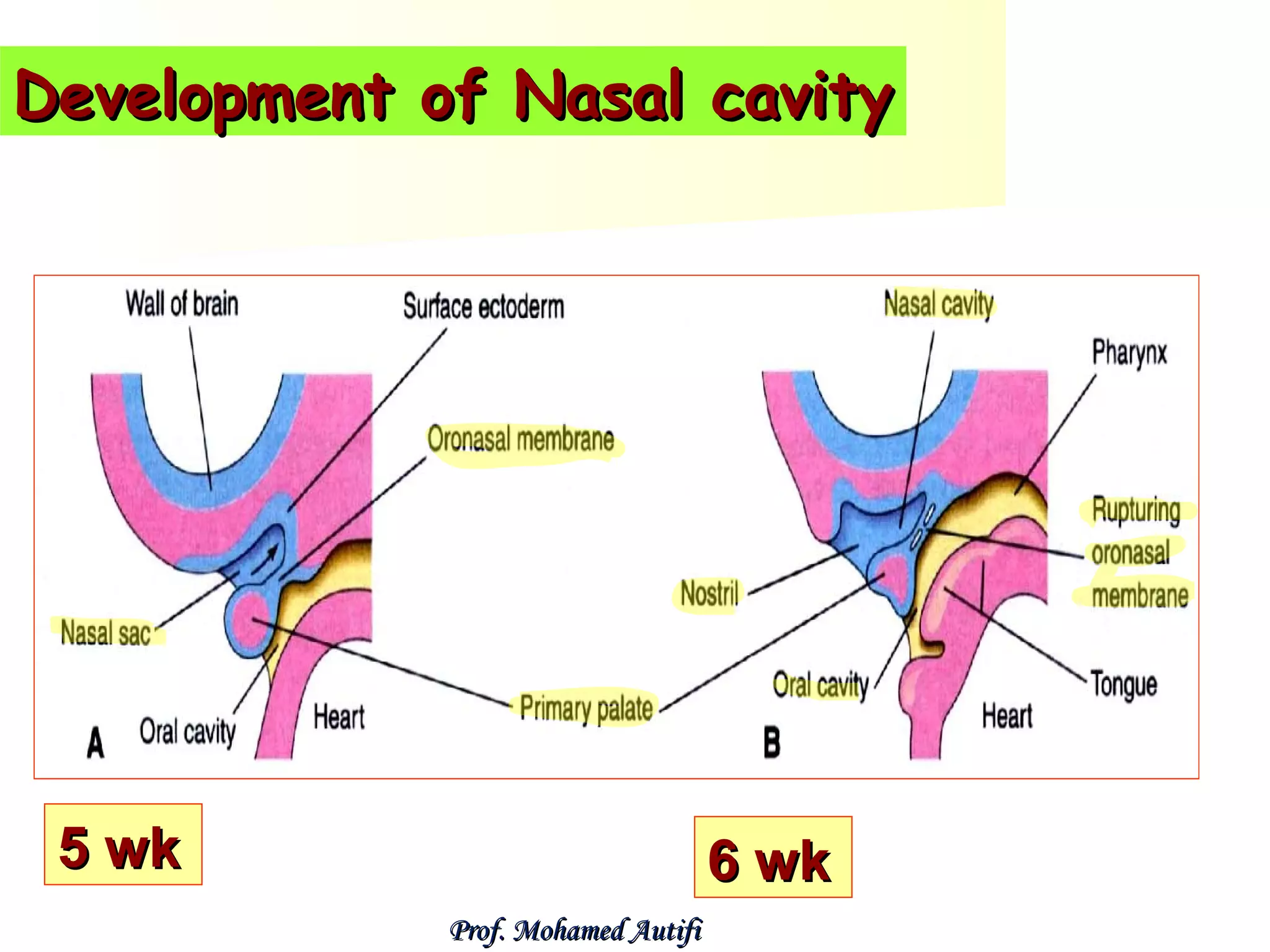
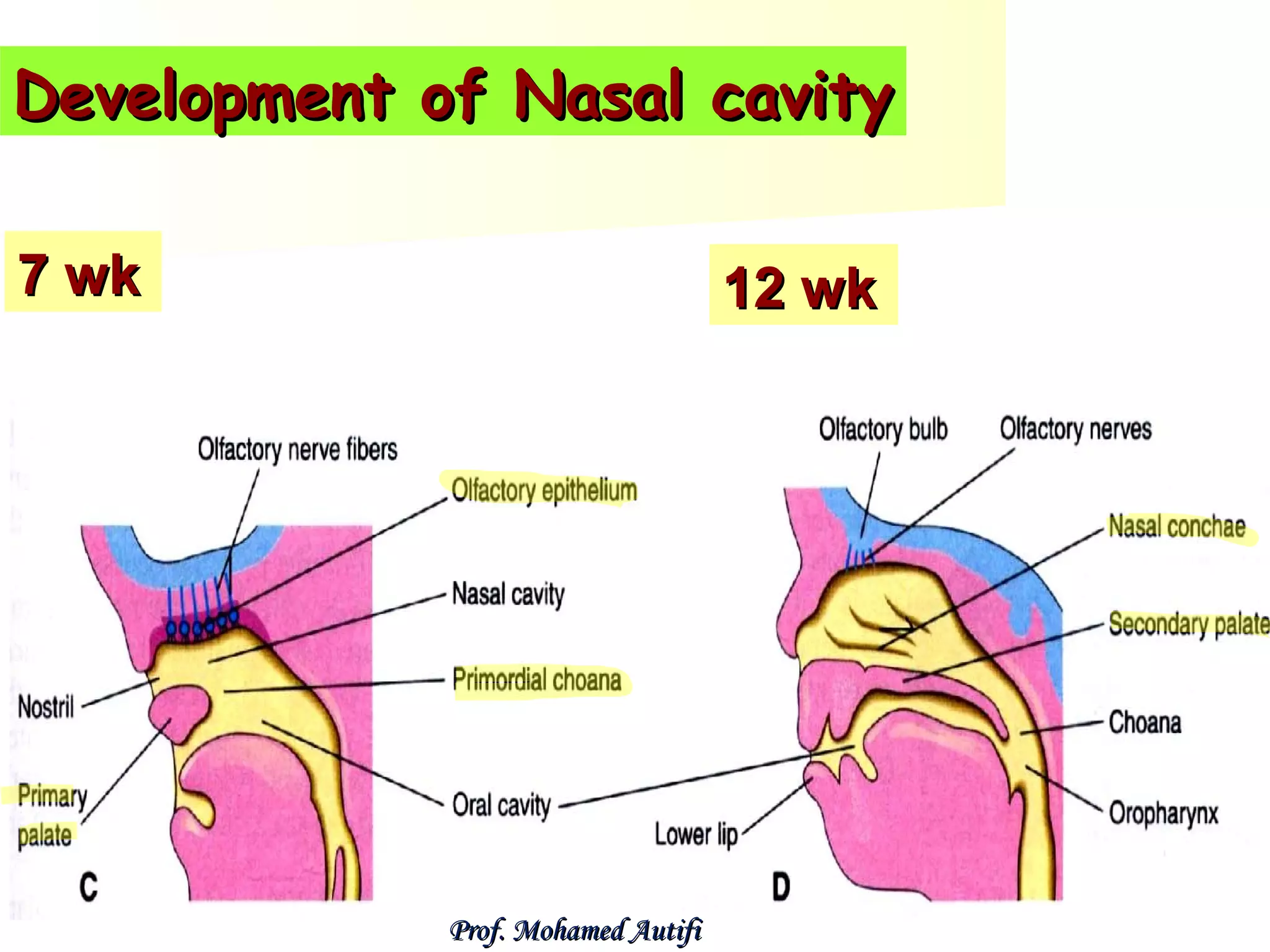
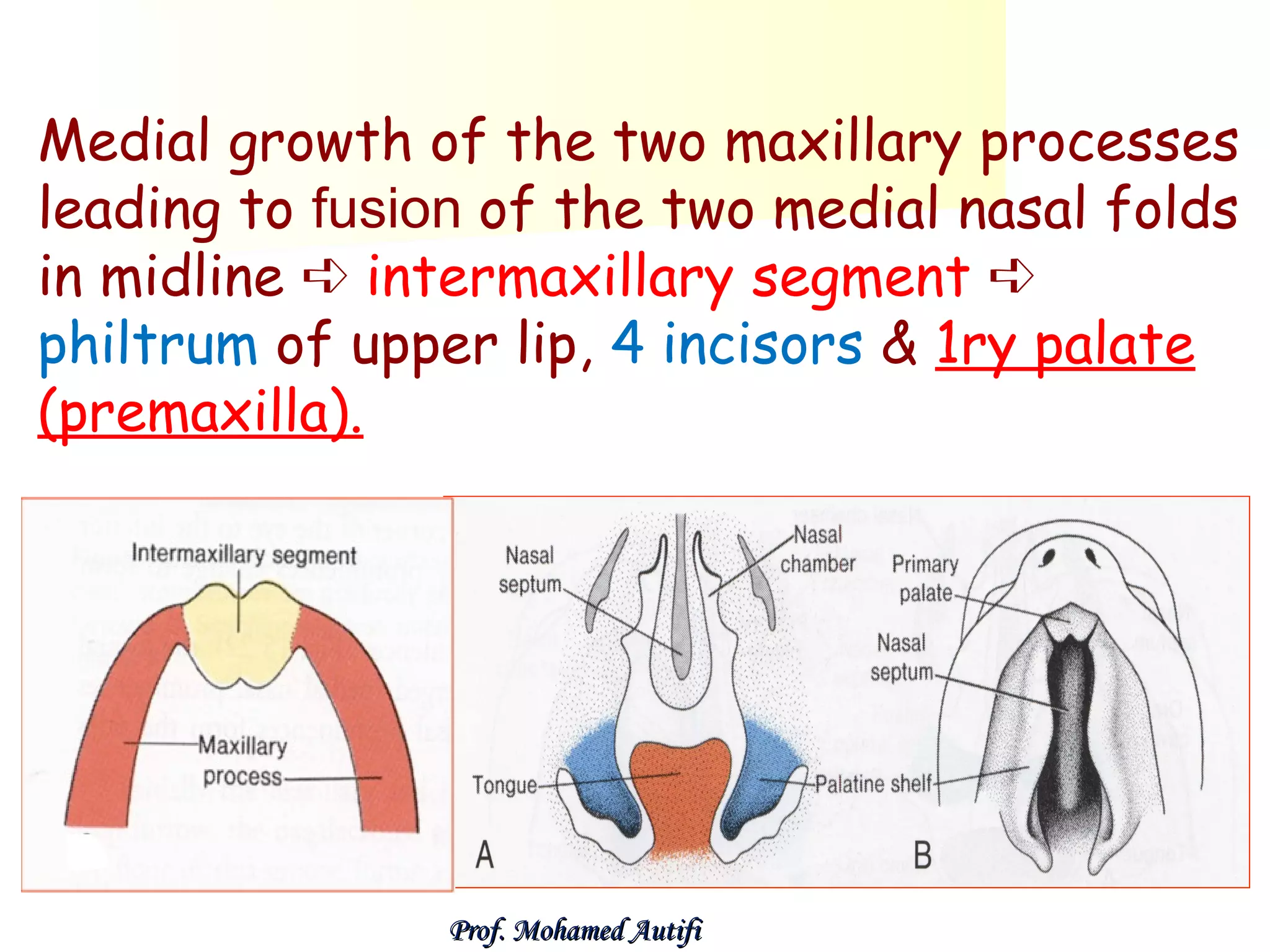
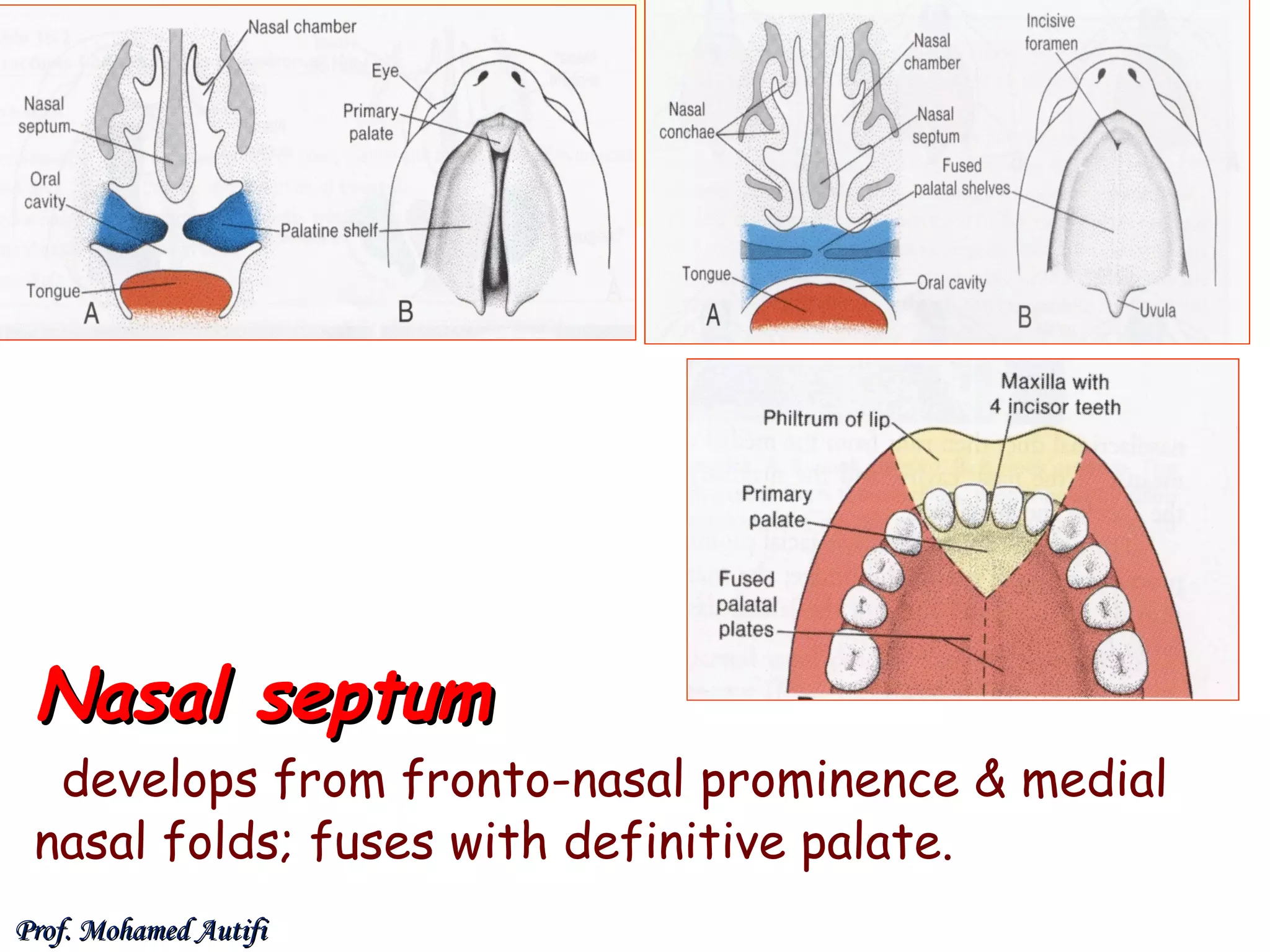
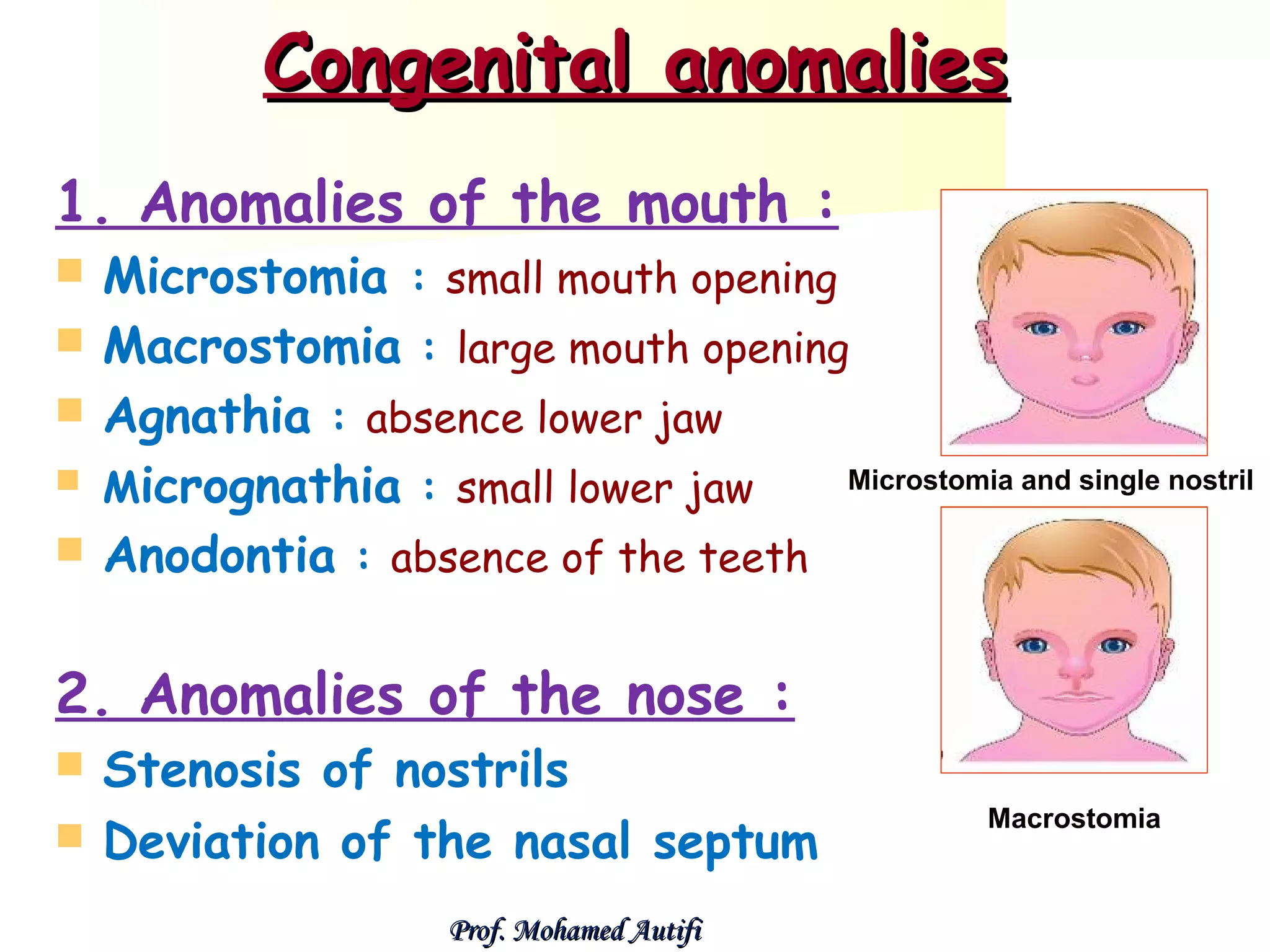
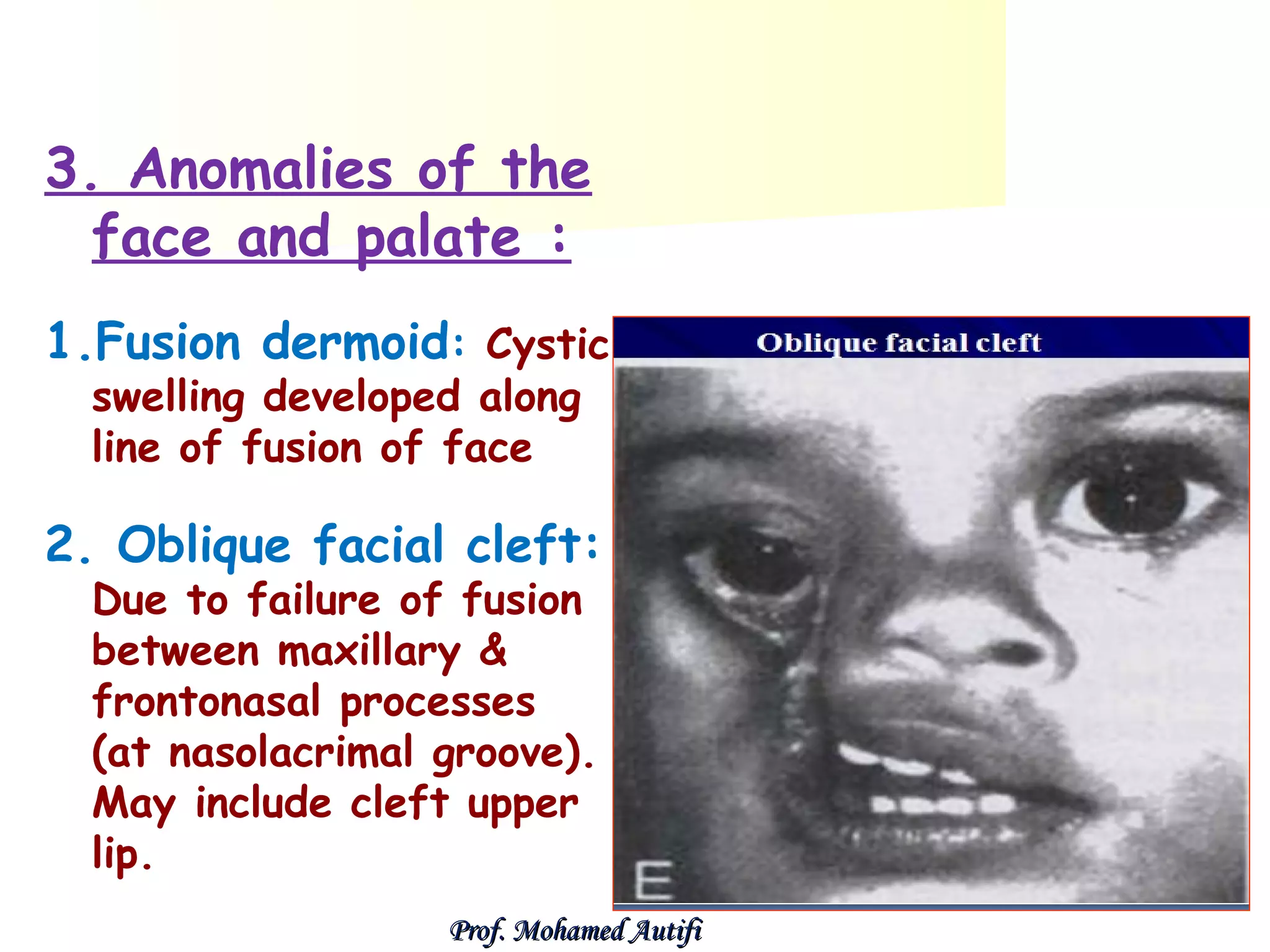
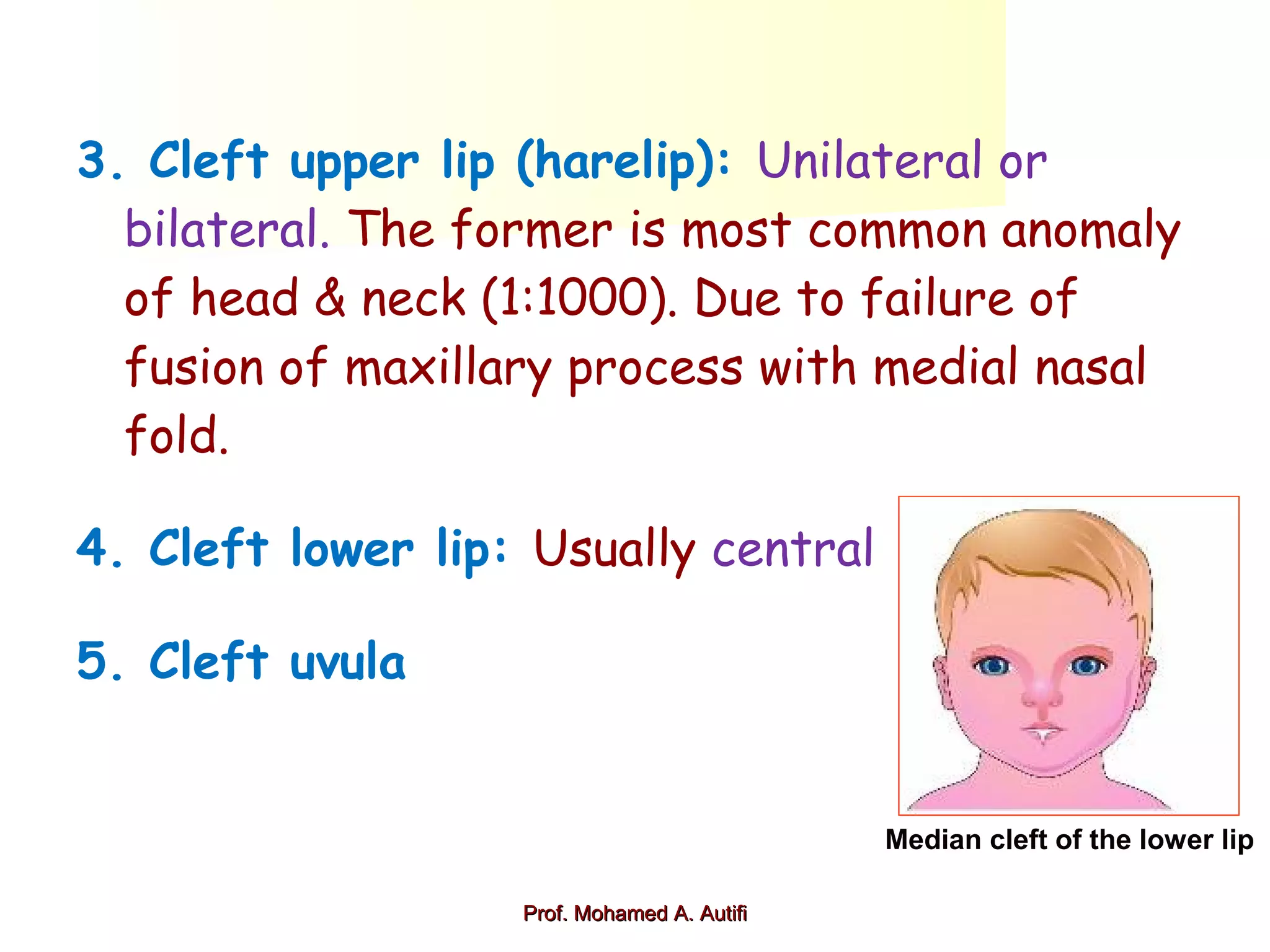
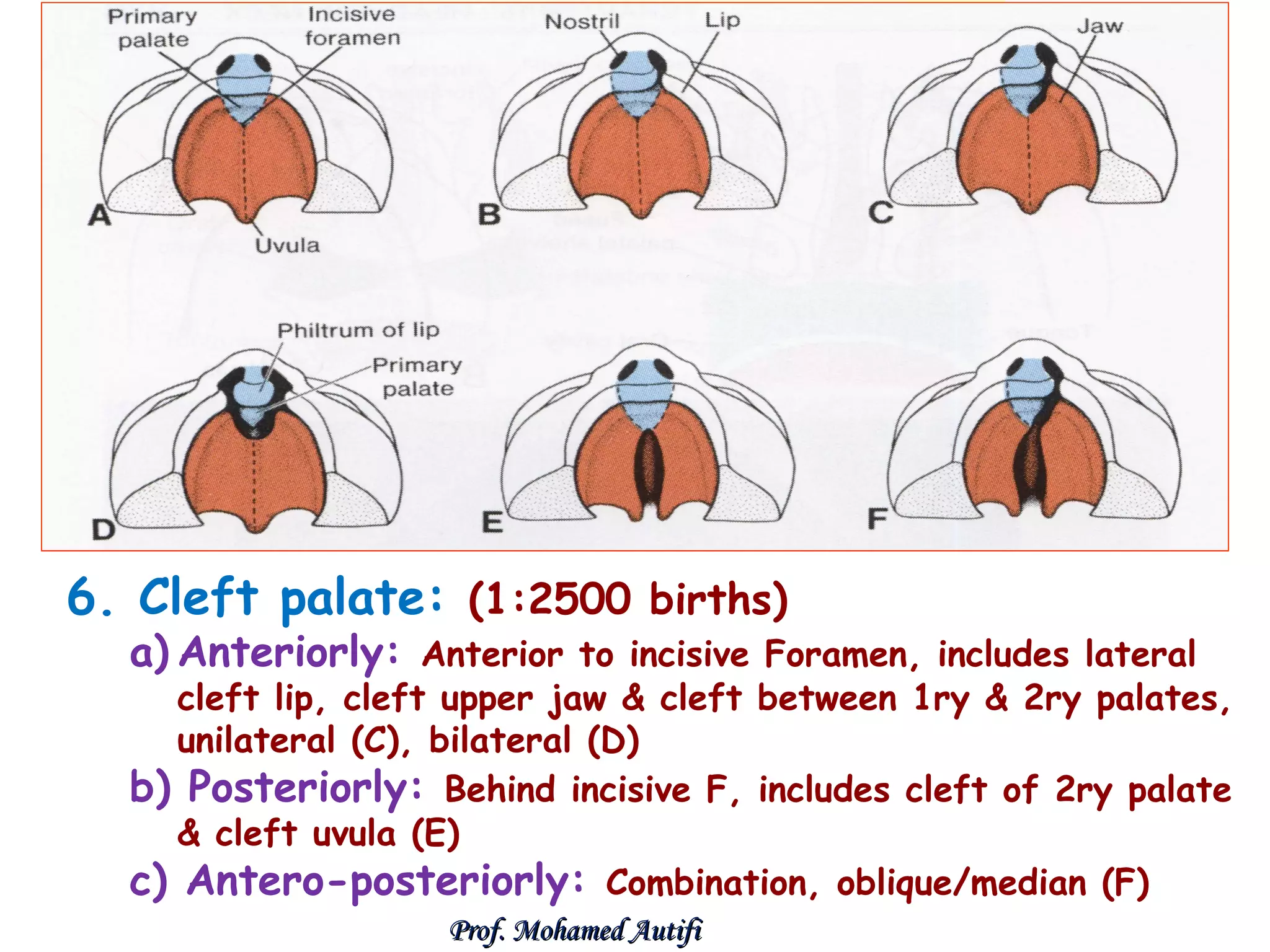
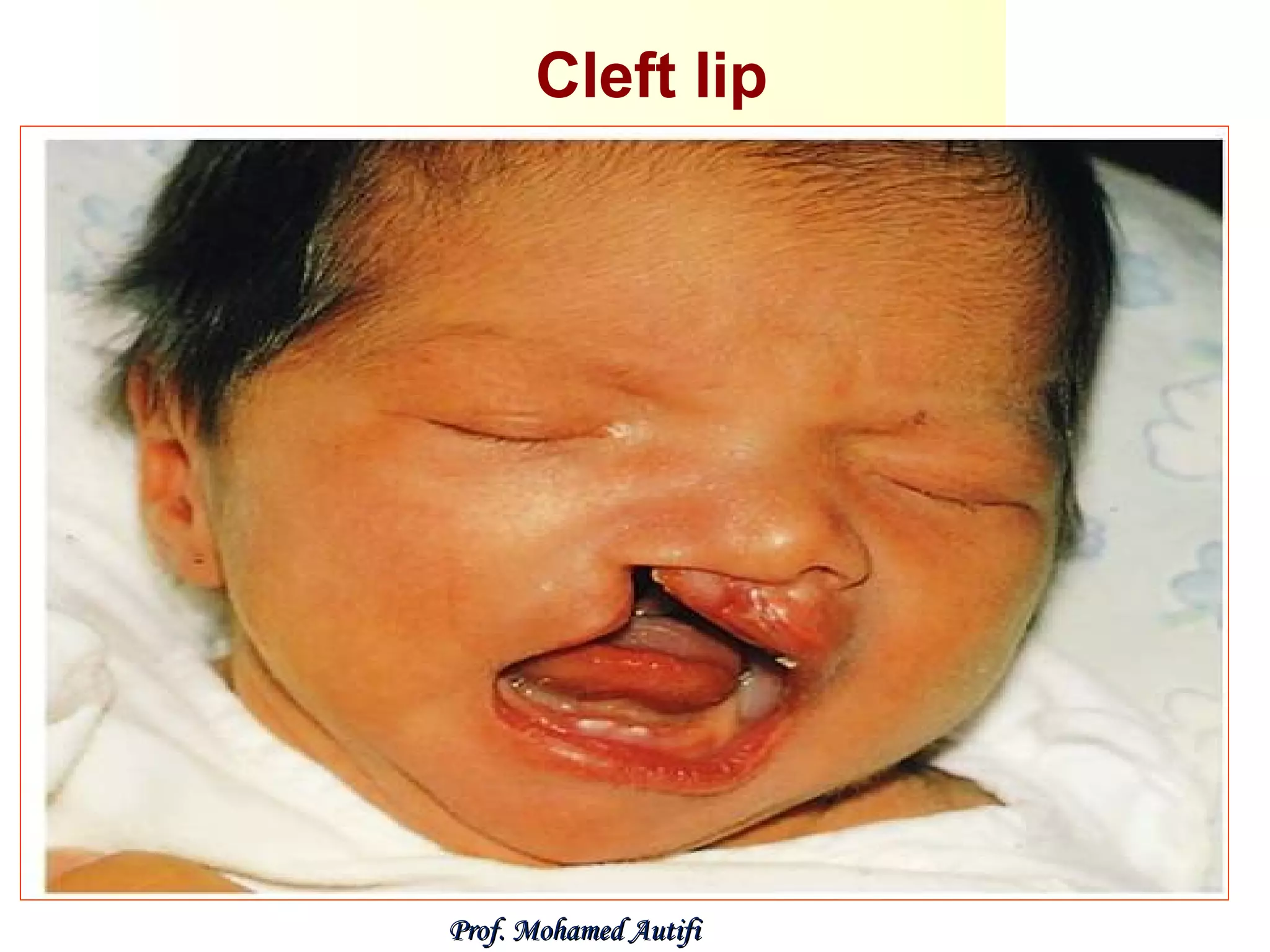
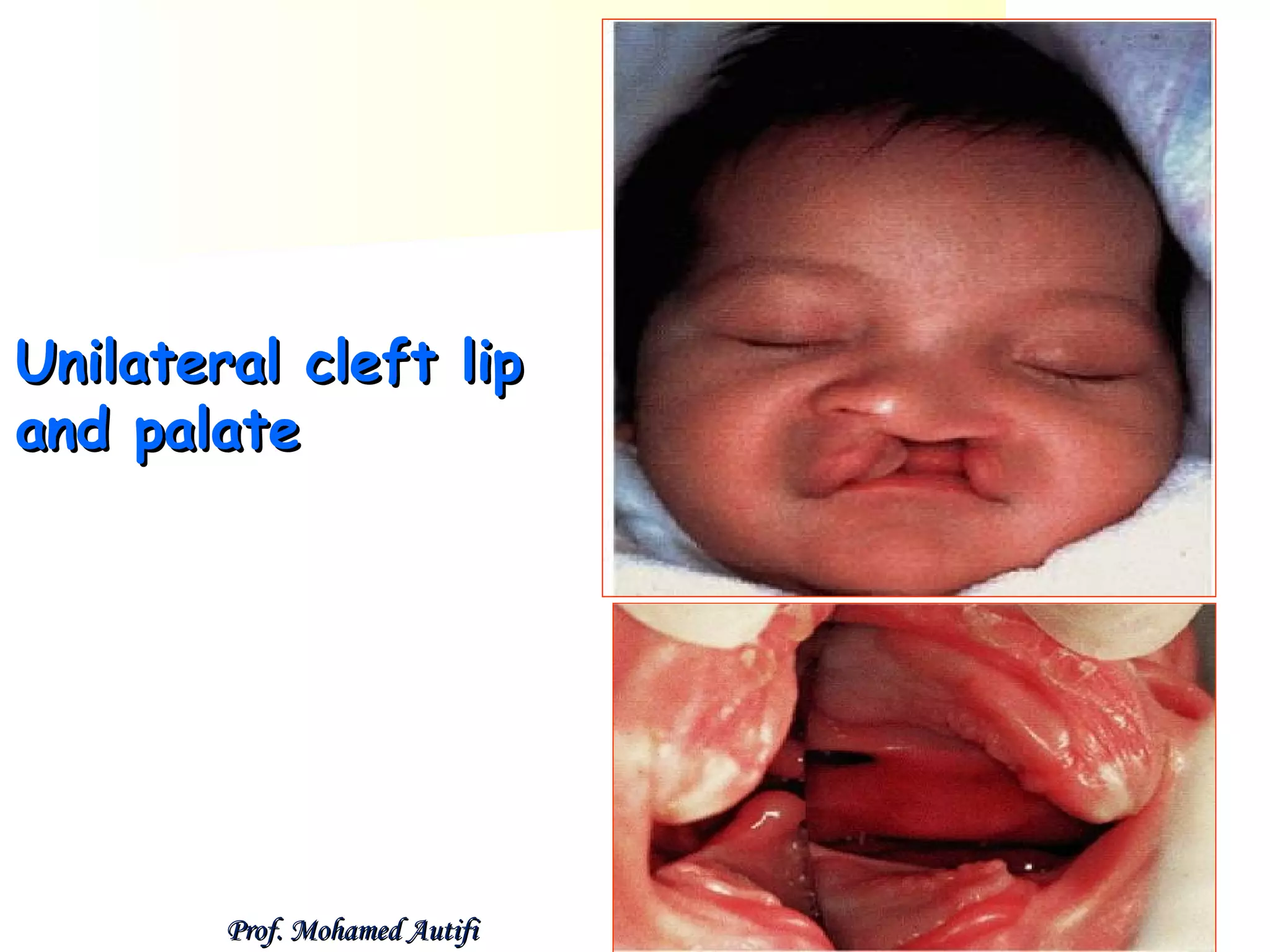
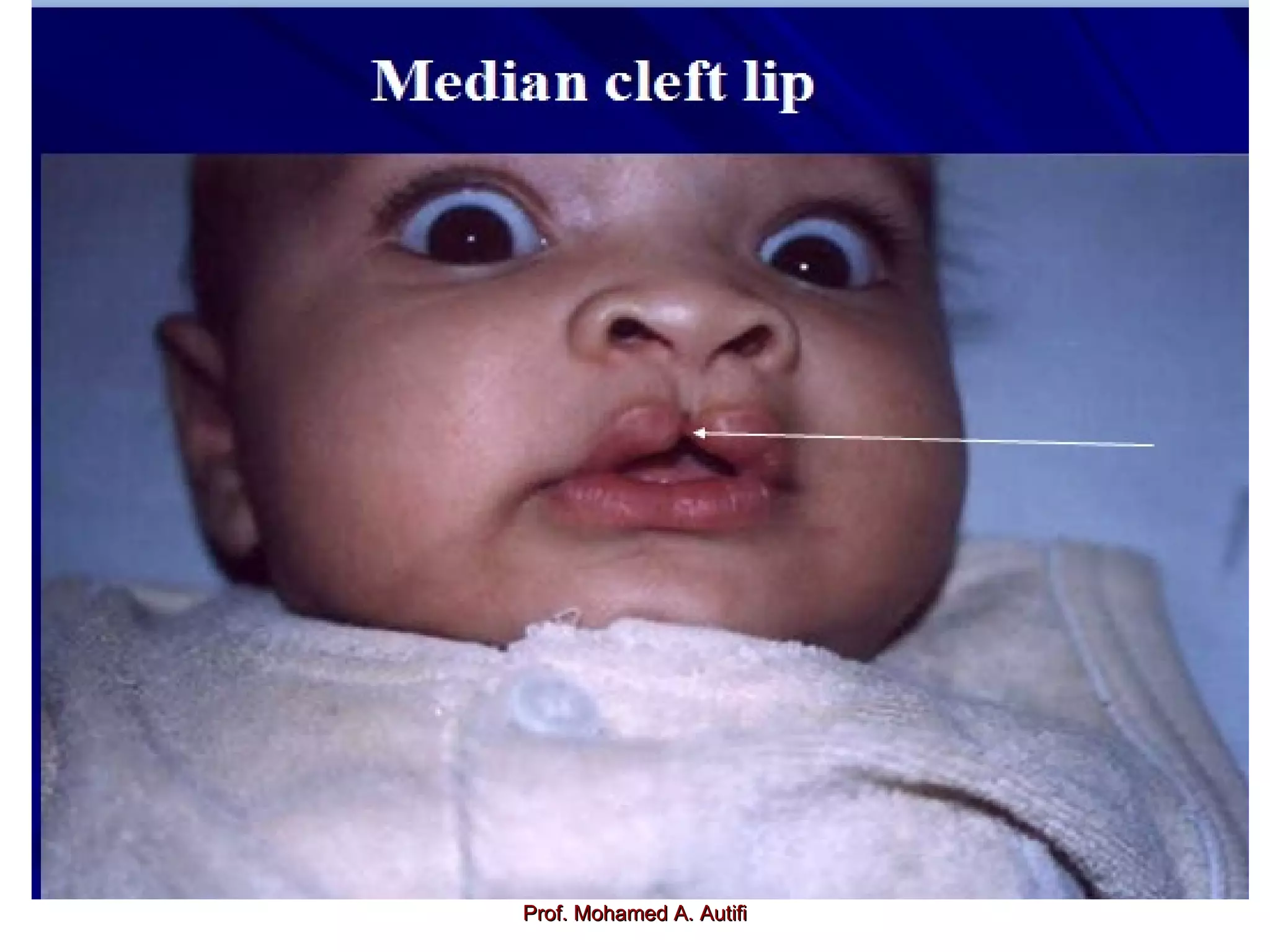
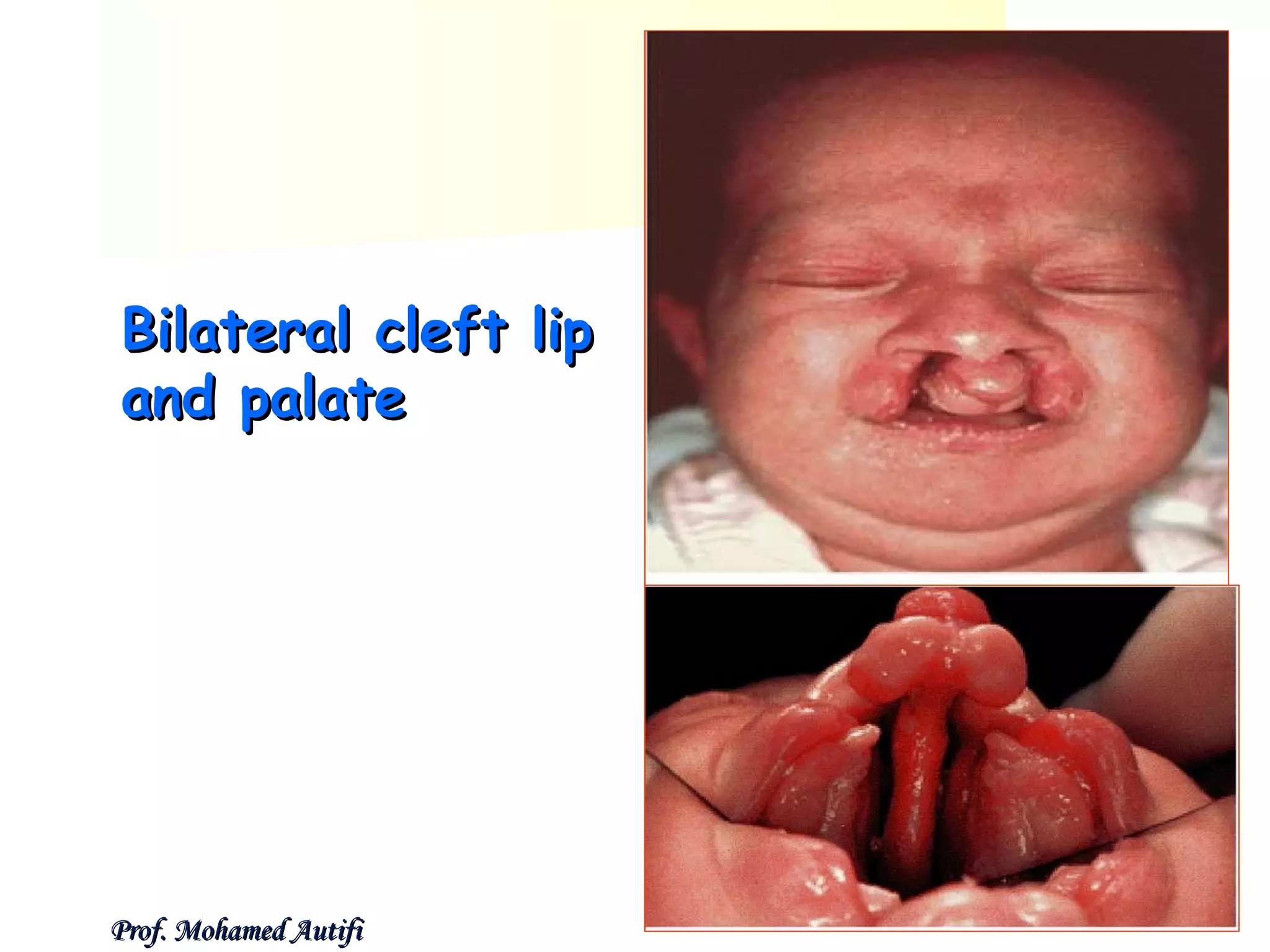
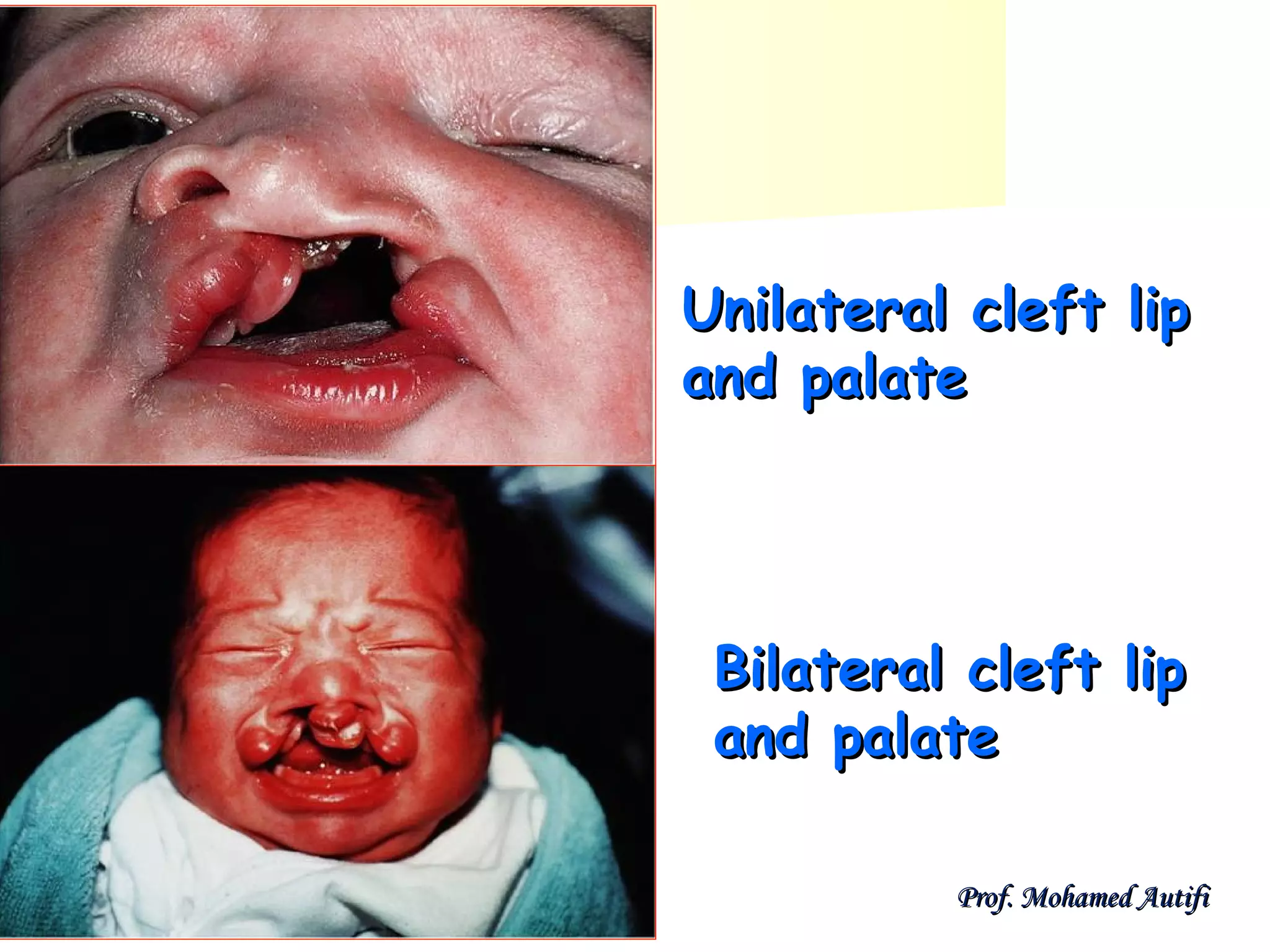
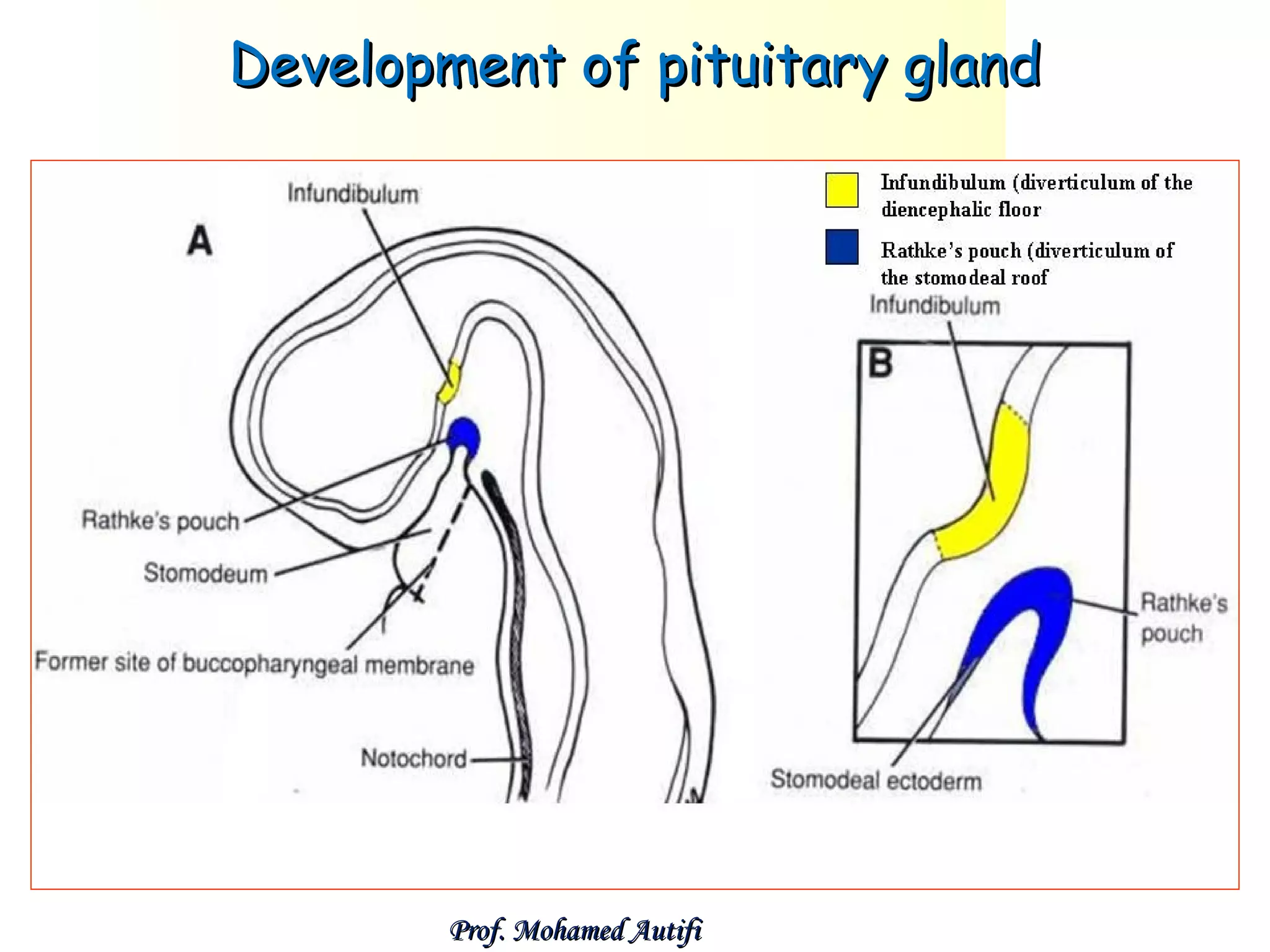
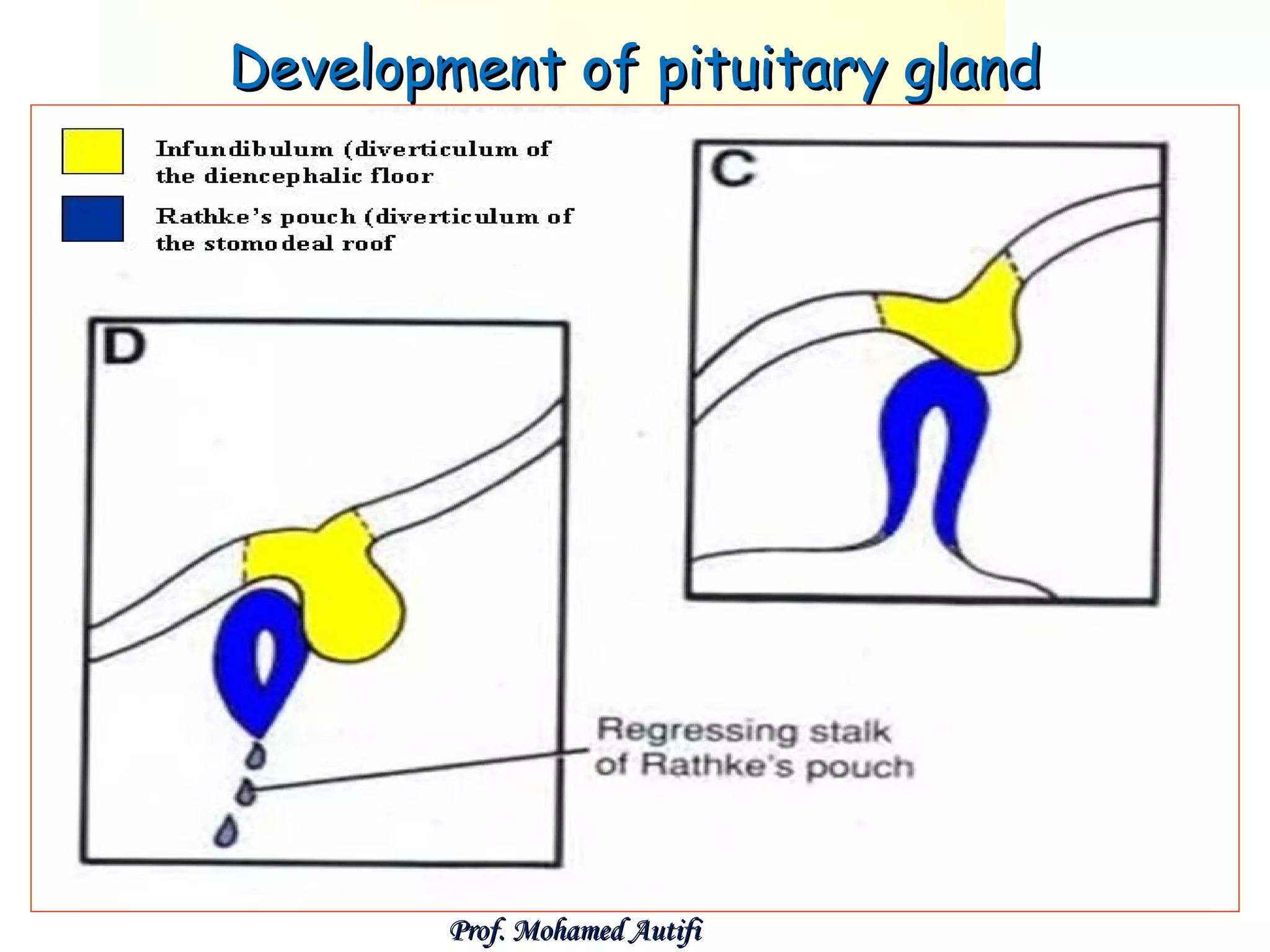
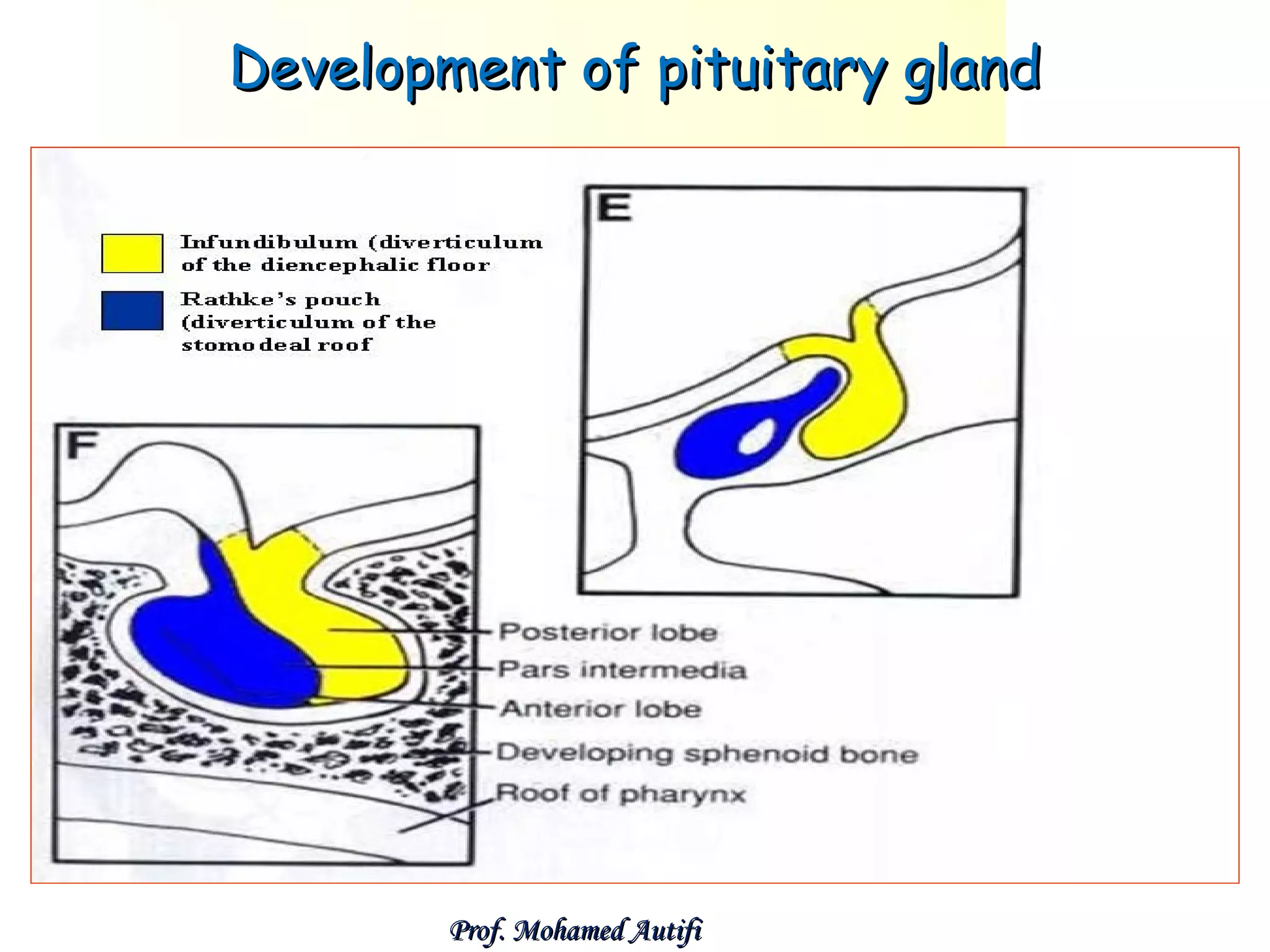
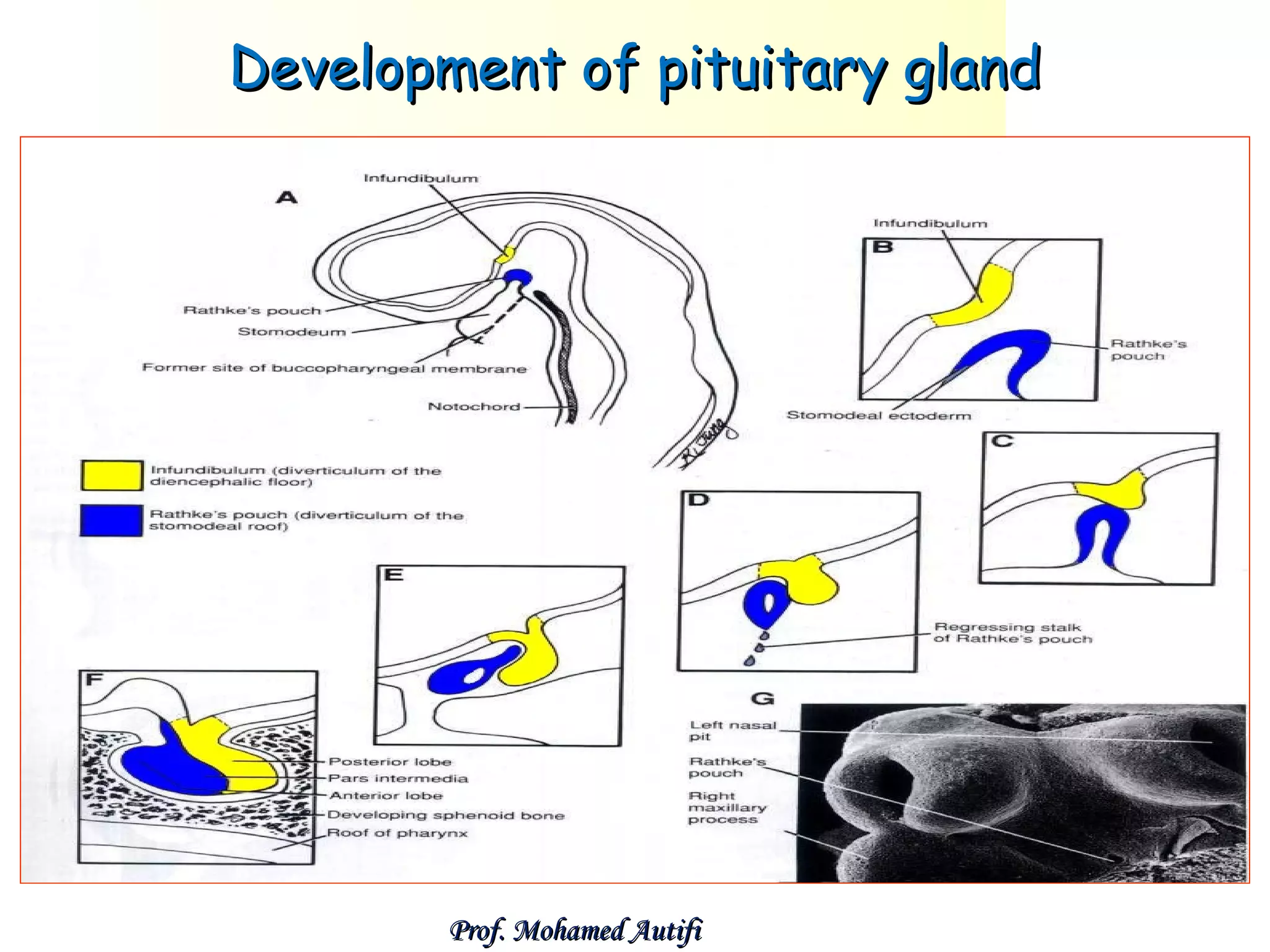

The document summarizes the development of the face, nose, palate, nasal cavities, and pituitary gland from the 4th week of development. It describes how the face develops from 5 mesenchymal prominences that surround the primitive mouth. It then discusses the development of specific structures such as the lips, salivary glands, nose, palate, and nasal cavities from these prominences. The pituitary gland is noted to develop from the ectoderm of the roof of the stomodeum and floor of the diencephalon. Some congenital anomalies are also briefly mentioned.



































































