phayrangeal apparatus By Dr.Aisha Sadaf IBMS -KMU-peshawar
•Download as PPTX, PDF•
15 likes•4,933 views

The document describes the development of the pharyngeal arches, pouches, and clefts in early human embryogenesis. It states that the pharyngeal arches develop as six curved mesenchymal thickenings on each side of the primitive pharynx. Each arch gives rise to specific skeletal, muscular, vascular and nervous derivatives. The pharyngeal pouches form as outpocketings between the arches and give rise to structures such as the tonsils and parathyroid glands. Pharyngeal clefts form between the pouches and contribute to structures like the external auditory meatus. Congenital anomalies can result if development of the arches, pouches or clefts is disrupted.

More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (16)
Similar to phayrangeal apparatus By Dr.Aisha Sadaf IBMS -KMU-peshawar
Similar to phayrangeal apparatus By Dr.Aisha Sadaf IBMS -KMU-peshawar (20)
phayrangeal apparatus By Dr.Aisha Sadaf IBMS -KMU-peshawar
- 2. INTRODUCTION After folding, the secondry yolk sac inside the embryo gives rise to:Fore gut-Mid gut–hind gut. The fore gut is divided into : a. Cranial part : extends from oral membrane to the laryngo-tracheal groove. It gives rise to : Part of mouth cavity Salivary glands Pharyngeal apparatus Respiratory system b. Caudal part : begins distal to the laryngotracheal groove. It gives rise to: esophagus-stomach- part of duodenum- liver-biliary system –pancreas. Amniotic cavity Oral membrane Gut Cloacal membrane Yolk sac Before folding Stomodeum Vitello-intestinal duct Allantois Cloacal membrane Hindgut Midgut Foregut Connecting stalk Amniotic cavity After folding
- 3. THE PHARYNGEAL ARCHES They are 6 curved cylindrical mesenchymal thickening on each side of the primitive pharynx. They develop in the head & neck similar in origin & structure to gills of the fish. Gill = Branchia Each arch consists of : 1. Outer ectodermal covering 2. Inner endodermal lining 3. Mesodermal core
- 4. Each pharyngeal arch consists, at first of mesenchyme derived from the lateral plate mesoderm. Soon, neural crest cells migrate into the pharyngeal arches and surround the central core of mesenchymal cells. Migration of neural crest cells into the arches produce discrete swelling demarcating each of the pharyngeal arch. NB. Mesenchyme =connective tissue of embryo The mesenchyme derived from neural crest cells is called (ectomesenchyme) to differentiate it from mesenchyme derived from mesoderm.
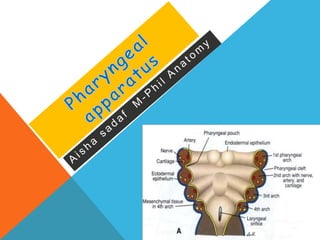
- 5. A typical pharyngeal arch contains: 1- A cartilaginous rod that forms the skeleton of the arch. 2- A muscular component that differentiates into muscles in the head and neck. 3- An aortic arch , an artery that arises from the truncus arteriosus of the primordial heart. 4- A nerve that supplies the mucosa and muscles derived from the arch.
- 6. NERVE SUPPLY OF THE PHARYNGEAL ARCHES It is derived from the hindbrain (pons and Medola oblogata) Each arch receives mixed nerve. Its motor branch supplies muscles derived from the arch. Its sensory branch supplies skin and mucous membrane of the arch.
- 7. DEVELOPMENT OF PHARYNGEAL ARCHES •By the end of the 4th week, 4 well defined pairs of pharyngeal arches are visible externally. •The 5th and 6th arches are small and cannot be seen on the surface of the embryo.
- 8. Most of the cartilages that form within the pharyngeal arches develop from the neural crest of the midbrain and hindbrain regions, although the cartilages of arches 4 and 6 apparently develop from lateral plate mesoderm. The first pharyngeal arch is remodeled to form a cranial maxillary process and a caudal mandibular process. Each process contains a central cartilaginous element (the maxillary is known as palato-pterygo-quadrate cartilage and the mandibular is known as Meckel's cartilage) surrounded by a mesenchymatic tissue. Cartilages
- 10. P R O F . M O H A M E D . A . A U T I F I Arch Skeletal Derivatives Muscular Derivatives Vascular Element Nerve First arch (mandibular arch) Consists of maxillary process and mandibular process Maxillary process gives rise to: 1. Maxilla 2. Zygomatic bone 3. Squamous part of temporal bone Mandibular process differentiates into : 1. Malleus 2. Incus 3. Anterior ligament of malleus 4. Spheno- mandibular ligament 5. Mandible 1.Muscles of Mastication 2.Tensor palati 3.Tensor tympani 4. Mylohoid 5. Anterior belly of digastric 1. Maxillary artery Mandibular nerve (V)
- 11. Derivatives of Cartilages of First Pharyngeal Arch The ventral part of the first arch cartilage ( Meckel cartilage ) form primordium of the mandible The middle part of cartilage forms anterior ligament of malleus and sphenomandibular ligament The dorsal end of first arch cartilage ossifies to form malleus and incus More details about cartilages
- 12. P R O F . M O H A M E D . A . A U T I F I Arch Skeletal Derivatives Muscular Derivatives Vascular Element Nerve Second arch (Hyoid arch) Reichert’s cartilage: Differentiates into: 1. Stapes 2. Styloid process 3. Stylohyoid ligament 4. LeSser horn of the hyoid bone 5. Superior(Uppe r)part of body of hyoid bone 1. Muscles of the scalp and face 2. Platysma 3. Stylohyoid 4. Stapedius 5. Posterior belly of digastric Stapedial Artery tympanic br. of ICA) Facial nerve (VII)
- 13. Derivatives of Cartilage of second Pharyngeal Arch The ventral end of second arch cartilage (Reichert cartilage) ossifies to form the lesser cornu and upper part of the body of the hyoid bone The dorsal end of second arch cartilage (Reichert cartilage) ossifies to form the stapes, styloid process and stylohyoid ligament
- 14. Arch Skeletal derivatives Muscular derivatives Vascular Element Nerve Third arch 1. Greater horn of hyoid bone 2. Lower part of body of hyoid bone Stylopharyngeus 1. I.C.A 2. C.C.A Glossopharyngeal nerve (IX) Fourth arch Thyroid cartilage Cricothyroid 1. Arch of aorta on left side 2. Subclavian A on right side Superior laryngeal nerve (X) Sixth arch Rest of Cartilages of the larynx except epiglottis: -Cricoid, -Arytenoid, -Corniculate and -Cuneiform. NB. The epiglottis develops from mesenchyme in hypobrancheal eminence 1. Other intrensic muscles of larynx 2. Constrector muscles of pharynx except Stylopharyngeus 3. Muscles of palate except tensor palati 1. Pulmonary A on each sides 2. Ductus arteriosus on left side Recurrent laryngeal nerve (X)
- 15. Derivatives of Third Pharyngeal Arch Cartilage The third arch cartilage ossifies to form the greater cornu and the lower part of the body of the hyoid bone
- 16. • The fourth and sixth arch cartilages fuse to form the laryngeal cartilages except epiglottis which develops from hypobrancheal eminence • The fifth pharyngeal arch is rudimentary and disappear later and has no derivatives Derivatives of The fourth and sixth Pharyngeal Arch Cartilages
- 19. DEVELOPMENT OF PHARYNGEAL POUCHES AND CLEFTS
- 20. PHARYNGEAL POUCHES The pharyngeal pouches are balloon-like diverticula that formed on the endodermal side between the pharyngeal arches The pairs of pouches develop in a craniocaudal sequence between the arches. The first pair of pouches lies between the first and second pharyngeal arches. There are four well defined pairs of pharyngeal pouches The fifth pair is absent or rudimentary •
- 21. It gives rise to tubotympanic recess which forms: 1.Tympanic cavity 2.Auditory tube. (pharyngotympanic tube or Eustachian tube) First pouch
- 22. • Gives rise to palatine tonsils • -Early in 3rd month, its lining epithelium proliferates ➪ solid tonsillar buds which grow into underlying mesoderm. • -Their central cells degenerate➪ hollow tonsillar crypts. • -Crypts & surrounding mesoderm ➪ palatine tonsils. • -Lymphatic tissue infiltrates its mesoderm during 3-5 Month • -Tonsillar capsule formed by condensed mesoderm. • -Remnants of pouch ➪ intratonsillar cleft Second pouch
- 23. Gives rise to: -inferior parathyroid glands. -thymus gland. At 6th week, they lose connection to pharyngeal wall. -Thymus gland migrates caudally & medially, pulling the parathyroid. The two thymic rudiments descend into thorax. Gland is large at time of birth, ➚ up to 2nd year, little ➚ until 7th year, rapid growth to 11th year, then ➘ to adult weight (12-15 gm) -Inferior parathyroid glands descends to lower pole of thyroid gland Third pouch
- 24. It gives rise to: 1.Superior parathyroid glands. It migrates with the thyroid gland. 2. Ultimo-branchial body. It incorporates into the thyroid gland. It gives parafollicular or C cells of thyroid gland Fourth pouch
- 25. PHARYNGEAL GROOVES (CLEFTS): In the 5th week: 4 clefts seen. The first cleft gives: external auditory meatus. The epithelium of the bottom forms outer layer of eardrum NB. Active growth of 2nd arch mesoderm overlaps 3rd & 4th arches. Temporarily, clefts ➪ectodermal cavity, cervical sinus, which disappears later.
- 26. DEVELOPMENT OF PHARYNGEAL POUCHES AND CLEFTS
- 29. 1. Branchial Cyst: Sinus persists as cyst along ant border of sternomastoid muscle. If ruptures ➪ branchial sinus 2. Branchial Sinus: a) External: Cyst opens outside, usually anterior to sternomastoid. b) Internal: Cyst opens into pharynx,usually in the tonsillar region. 3. Cervical Fistula: Sinus opens externally & internally, connects pharynx with outside. Congenital anomalies
- 30. 4. 1st Arch Syndrome (Mandibulofacial dystosis) Maldevelopment of components of 1st pharyngeal arch results in various congenital malformations of eyes, ears, mandible and palate. This is due to failures of Proper neural crest migration into the 1st branchial arches. 5. DiGeorge Syndrome. Improper migration of neural crest cells into the 3rd and 4th branchial arches. It is characterized by: 1.Minor deformations of the lower face. 2.Thymic and parathyroid aplasia (i.e., no thymus and no parathyroids). The absence of a thymus has a very deleterious effect on the development of the immune system. The absence of parathyroids leads to hypocalcemia. 3.Problems with aorticopulmonary septation. Congenital anomalies
- 31. 6. Ectopic Thymic Tissue: Thymus gland lies in the neck. 7. Ectopic Parathyroid: Inferior parathyroid may present at bifurcation of Common carotid artery. Congenital anomalies