Downloaded 1,546 times



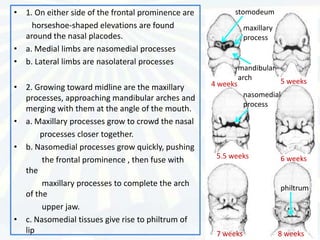
![Introduction
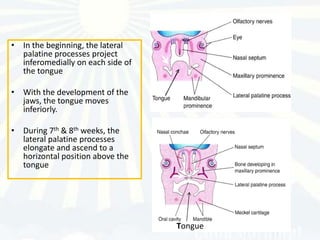
• The embryonic period extends from the
beginning of the fourth week till the end of the
eighth week.
• The trilaminar embryonic area differentiates as
follows:
1] ectoderm providing protection,
2] endoderm providing nutrition ,
3] mesoderm forming skeletal tissue ,muscle and
blood vascular system
• The fourth week is characterized by the
differentiation of the three germ layers and the
folding of the embryo
• In the second month the organs and tissues are
laid down and the embryo has a distinct human
appearance](https://image.slidesharecdn.com/developmentofface-130114013510-phpapp02/85/Development-of-face-4-320.jpg)



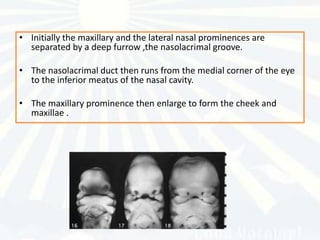




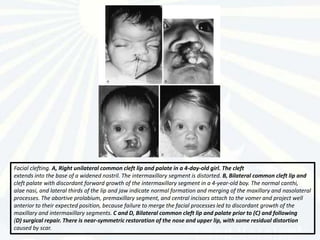
![Facial clefting. A, Absence of the intermaxillary segment with hypotelorism. The maxillary
processes form the normal lateral thirds of the upper lips. The midline rectangular defect indicates the site of the
deficient intermaxillary segment with absent prolabium, incisors, and primary palate. There was consequent clefting
of the secondary palate. Absent intermaxillary segment with hypotelorism signifies a high likelihood of
holoprosencephaly. B, True midline cleft of the upper lip and philtrum with hypertelorism. The nose is normal. A
7-month-old girl with transethmoidal cephalocele and left optic nerve dysplasia (morning glory syndrome). True
midline cleft lip signifies the high likelikhood of midline craniofaciocerebral and optic dysraphysm. C and D,
Midline cleft lip is also found in association with Mohr syndrome (orofacial digital syndrome II [OFD II]). The
presence of reduplicated great toes bilaterally helps to identify OFD II and to distinguish it from OFD I.](https://image.slidesharecdn.com/developmentofface-130114013510-phpapp02/85/Development-of-face-78-320.jpg)


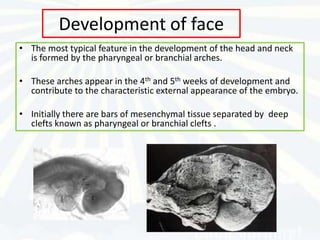
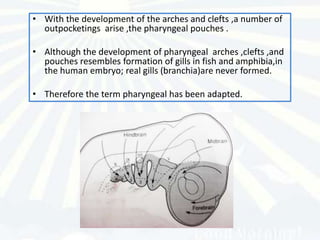
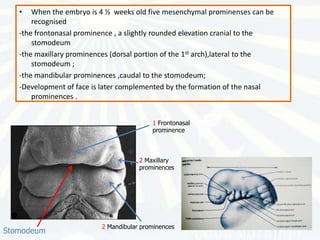
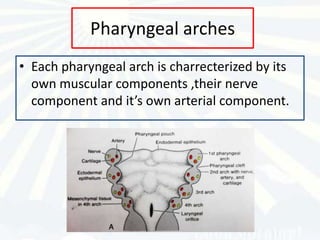
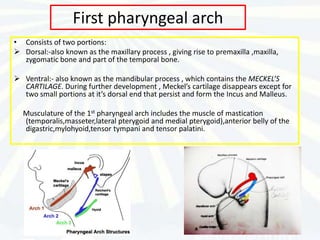
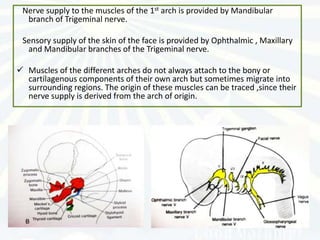
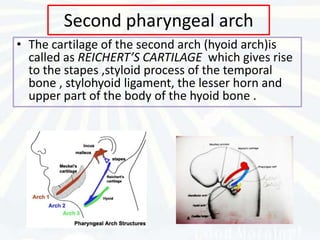
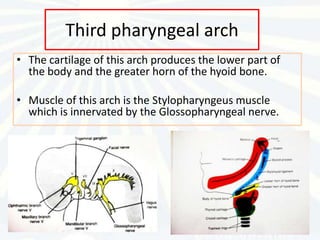
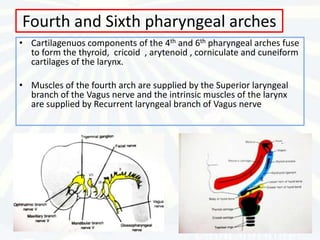
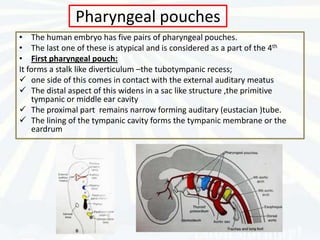
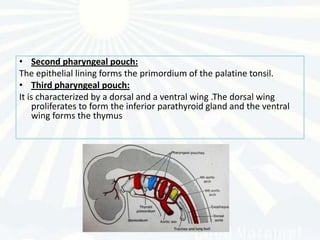
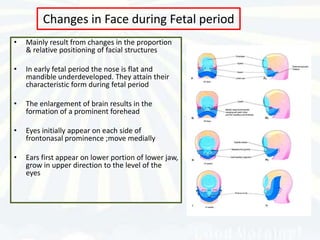
The document summarizes the development of the face from the 4th week of embryonic development. It discusses how the frontonasal prominence, maxillary prominences, and mandibular prominences form the basic structures of the face. It describes the development of specific structures like the nose, palate, ears, eyes, lips, and tongue from these prominences. It also discusses the theories of craniofacial growth and the role of the pharyngeal arches, pouches, grooves, and clefts in facial development.





























































































